Fill a Valid Ada Dental Claim Form
Fill a Valid Ada Dental Claim Form
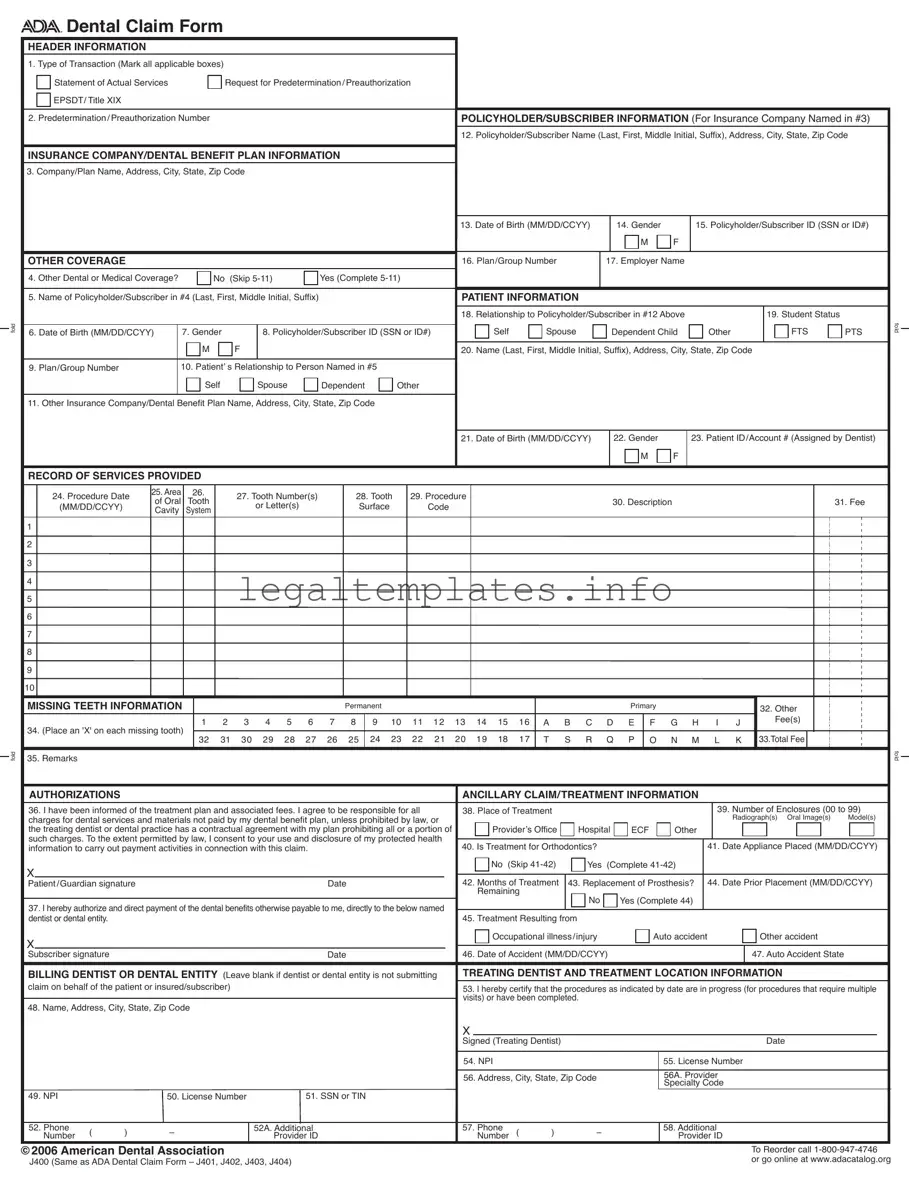
The ADA Dental Claim Form is a critical tool used by dental professionals and patients alike to document dental services and submit dental insurance claims. With spaces dedicated to capturing comprehensive information about the patient, the policyholder, and the dental provider, this form facilitates the processing of dental claims by insurance companies. It includes details such as the type of transaction, policyholder and patient information, details of the dental procedure performed, and any additional coverage that may be relevant. The form also requires the patient's authorization, acknowledging their understanding of the treatment plan and associated costs not covered by insurance. Designed for clarity and efficiency, the ADA Dental Claim Form must be filled out with care to ensure all transactions are processed smoothly. Instructions for filling out the form emphasize completeness and accuracy, making it imperative for users to be meticulous in providing all necessary details. Featuring sections for the identification of the billing dentist or dental entity, along with specific codes for dental specialties, the form is a comprehensive document that supports the administrative side of dental care. Understanding how to properly complete and utilize the ADA Dental Claim Form can significantly impact the timely and successful reimbursement of dental services.
fold
fold



 Dental Claim Form
Dental Claim Form
HEADER INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Type of Transaction (Mark all applicable boxes) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Statement of Actual Services |
|
|
Request for Predetermination/Preauthorization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
EPSDT/ Title XIX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Predetermination/Preauthorization Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLICYHOLDER/SUBSCRIBER INFORMATION (For Insurance Company Named in #3) |
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
12. Policyholder/Subscriber Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
INSURANCE COMPANY/DENTAL BENEFIT PLAN INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Company/Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. Date of Birth (MM/DD/CCYY) |
|
|
14. Gender |
|
|
15. Policyholder/Subscriber ID (SSN or ID#) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
OTHER COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16. Plan/Group Number |
|
|
17. Employer Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
4. Other Dental or Medical Coverage? |
|
|
No (Skip |
|
|
Yes (Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
5. Name of Policyholder/Subscriber in #4 (Last, First, Middle Initial, Suffix) |
|
|
|
|
|
|
|
PATIENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. Relationship to Policyholder/Subscriber in #12 Above |
|
|
|
|
|
|
|
19. Student Status |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Self |
|
Spouse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FTS |
PTS |
fold |
|||||||||
6. Date of Birth (MM/DD/CCYY) |
|
7. Gender |
|
|
|
8. Policyholder/Subscriber ID (SSN or ID#) |
|
|
|
Dependent Child |
Other |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
M |
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20. Name (Last, First, Middle Initial, Suffix), Address, City, State, Zip Code |
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
9. Plan/Group Number |
|
|
10. Patient’ s Relationship to Person Named in #5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
Self |
|
|
|
Spouse |
|
Dependent |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
11. Other Insurance Company/Dental Benefit Plan Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. Date of Birth (MM/DD/CCYY) |
|
|
22. Gender |
|
|
23. Patient ID/Account # (Assigned by Dentist) |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
RECORD OF SERVICES PROVIDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
24. Procedure Date |
25. Area |
26. |
|
27. Tooth Number(s) |
|
|
28. Tooth |
29. Procedure |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
of Oral |
Tooth |
|
|
|
|
|
|
|
|
|
30. Description |
|
|
|
|
|
|
|
|
|
|
|
31. Fee |
|
||||||||||||||||||||||||||||
|
(MM/DD/CCYY) |
|
|
|
|
or Letter(s) |
|
|
|
Surface |
Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
Cavity |
System |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MISSING TEETH INFORMATION |
|
|
|
|
|
|
|
|
|
|
Permanent |
|
|
|
|
|
|
|
|
|
|
Primary |
|
|
|
|
|
|
|
|
|
32. Other |
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
8 |
|
9 10 11 12 13 14 15 16 |
A B C D E |
F G H |
|
I |
J |
|
|
|
|
Fee(s) |
|
|
|
|
|
|
|
|||||||||||||||||||
34. (Place an 'X' on each missing tooth) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
32 |
31 |
30 |
29 |
28 |
27 |
26 |
|
25 |
|
24 23 |
22 21 |
|
20 19 18 |
17 |
T |
S R |
Q |
P |
O |
N M |
|
L |
K 33.Total Fee |
|
|
|
|
|
|
|
||||||||||||||||
35. Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fold |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
AUTHORIZATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ANCILLARY CLAIM/TREATMENT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
36. I have been informed of the treatment plan and associated fees. I agree to be responsible for all |
38. Place of Treatment |
|
|
|
|
|
|
|
|
|
|
|
|
39. Number of Enclosures (00 to 99) |
|
||||||||||||||||||||||||||||||||||||||
charges for dental services and materials not paid by my dental benefit plan, unless prohibited by law, or |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Radiograph(s) Oral Image(s) |
Model(s) |
|
|||||||||||||||||||||||||||||||||
the treating dentist or dental practice has a contractual agreement with my plan prohibiting all or a portion of |
|
Provider’s Office |
Hospital |
ECF |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
such charges. To the extent permitted by law, I consent to your use and disclosure of my protected health |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
information to carry out payment activities in connection with this claim. |
|
|
|
|
|
|
|
40. Is Treatment for Orthodontics? |
|
|
|
|
|
|
|
|
|
41. Date Appliance Placed (MM/DD/CCYY) |
|
||||||||||||||||||||||||||||||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No (Skip |
Yes |
(Complete |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Guardian signature |
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
42. Months of Treatment |
43. Replacement of Prosthesis? |
|
44. Date Prior Placement (MM/DD/CCYY) |
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remaining |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
37. I hereby authorize and direct payment of the dental benefits otherwise payable to me, directly to the below named |
|
|
|
|
No |
|
|
Yes (Complete 44) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
dentist or dental entity. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. Treatment Resulting from |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Occupational illness/injury |
|
|
|
Auto accident |
|
|
|
|
|
Other accident |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Subscriber signature |
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
46. Date of Accident (MM/DD/CCYY) |
|
|
|
|
|
|
|
|
|
|
47. Auto Accident State |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
BILLING DENTIST OR DENTAL ENTITY (Leave blank if dentist or dental entity is not submitting |
TREATING DENTIST AND TREATMENT LOCATION INFORMATION |
|
|
|
|
|
|||||||||||||||||||||||||||||||||||||||||||||||
claim on behalf of the patient or insured/subscriber) |
|
|
|
|
|
|
|
|
|
|
|
|
|
53. I hereby certify that the procedures as indicated by date are in progress (for procedures that require multiple |
|
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
visits) or have been completed. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
48. Name, Address, City, State, Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signed (Treating Dentist) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
54. NPI |
|
|
|
|
|
|
|
|
|
55. License Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
56. Address, City, State, Zip Code |
|
|
|
|
|
56A. Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
49. NPI |
|
|
50. License Number |
|
|
|
51. SSN or TIN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
52. Phone |
( |
) |
– |
|
|
|
|
|
52A. Additional |
|
|
|
|
|
|
|
57. Phone |
( |
) |
– |
|
|
|
|
|
58. Additional |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Number |
|
|
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
Provider ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
©2006 American Dental Association |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
To Reorder call |
|
||||||||||||||||||||
J400 (Same as ADA Dental Claim Form – J401, J402, J403, J404) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or go online at www.adacatalog.org |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||

Comprehensive completion instructions for the ADA Dental Claim Form are found in Section 4 of the ADA Publication titled
GENERAL INSTRUCTIONS
A. The form is designed so that the name and address (Item 3) of the
B. In the
assignment of a claim or control number.
|
C. All Items in the form must be completed unless it is noted on the form or in the following instructions that completion is not required. |
|
|
D. When a name and address field is required, the full name of an individual or a full business name, address and zip code must be entered. |
|
|
E. All dates must include the |
|
|
F. If the number of procedures reported exceeds the number of lines available on one claim form, the remaining procedures must be |
|
listed on a separate, fully completed claim form. |
|
COORDINATION OF BENEFITS (COB)
When a claim is being submitted to the secondary payer, complete the form in its entirety and attach the primary payer’s Explanation of Benefits (EOB) showing the amount paid by the primary payer. You may indicate the amount the primary carrier paid in the “Remarks” field (Item # 35).
NATIONAL PROVIDER IDENTIFIER (NPI)
49 and 54 NPI (National Provider Indentifier): This is an identifier assigned by the Federal government to all providers considered to be HIPAA covered entities. Dentists who are not covered entities may elect to obtain an NPI at their discretion, or may be enumerated if required by a participating provider agreement with a
ADDITIONAL PROVIDER IDENTIFIER
52A and 58 Additional Provider ID: This is an identifier assigned to the billing dentist or dental entity other than a Social Security Number (SSN) or Tax Identification Number (TIN). It is not the provider’s NPI. The additional identifier is sometimes referred to as a Legacy Identifier (LID). LIDs may not be unique as they are assigned by different entities (e.g.,
PROVIDER SPECIALTY CODES
56A Provider Specialty Code: Enter the code that indicates the type of dental professional who delivered the treatment. Available codes describing treating dentists are listed below. The general code listed as ‘Dentist’ may be used instead of any other dental practitioner code.
Category / Description Code |
Code |
|
|
Dentist |
|
A dentist is a person qualified by a doctorate in dental surgery (D.D.S) |
122300000X |
or dental medicine (D.M.D.) licensed by the state to practice dentistry, |
|
and practicing within the scope of that license. |
|
|
|
General Practice |
1223G0001X |
Dental Specialty (see following list) |
Various |
Dental Public Health |
1223D0001X |
Endodontics |
1223E0200X |
Orthodontics |
1223X0400X |
Pediatric Dentistry |
1223P0221X |
Periodontics |
1223P0300X |
Prosthodontics |
1223P0700X |
Oral & Maxillofacial Pathology |
1223P0106X |
Oral & Maxillofacial Radiology |
1223D0008X |
Oral & Maxillofacial Surgery |
1223S0112X |
Dental provider taxonomy codes listed above are a subset of the full code set that is posted at:
Should there be any updates to ADA Dental Claim Form completion instructions, the updates will be posted on the ADA’s web site at:
www.ada.org/goto/dentalcode
| Fact Name | Description |
|---|---|
| Form Identification | The document is recognized as the ADA Dental Claim Form, also known as J400. |
| Design Purpose | Designed for the easy visibility of the insurance company or dental benefit plan's name and address in a standard #10 window envelope when folded properly. |
| Mandatory Completion | All items on the form must be completed unless specified otherwise on the form or in its instructions. |
| Procedure Date Requirement | Every date entered on this form must include the four-digit year. |
| National Provider Identifier (NPI) | This is a unique identifier assigned by the federal government to healthcare providers, including dentists, covered by HIPAA. |
| Additional Provider Identifier | Refers to any identifier assigned to the billing dentist or dental entity other than the Social Security Number (SSN) or Tax Identification Number (TIN), not including the provider’s NPI. |
Filling out an ADA Dental Claim form accurately is crucial for ensuring prompt and correct payment for dental services rendered. This step-by-step guide will help you complete the form methodically, minimizing the chances of rejection due to errors or omissions. Remember, each section of the form plays an important role in the claim process, from providing personal and insurance information to detailing the services provided. Let's begin.
Review the completed form for accuracy before submitting it to ensure it complies with all requirements. This meticulous approach helps in preventing delays in processing and ensures that the claim is addressed efficiently by the insurance company. Remember, completing the ADA Dental Claim Form accurately is a vital step towards successful reimbursement for dental services.
What is the ADA Dental Claim Form used for?
The ADA Dental Claim Form is utilized for submitting dental claims to insurance companies or dental benefit plans. It is designed to document the treatment received by a patient and request reimbursement from the relevant insurance company or dental benefit plan. This form covers a range of details, including types of transactions, policyholder/subscriber information, patient information, details of the service provided, and authorization for the insurer to pay the dental provider directly.
How do you fill out the ADA Dental Claim Form correctly?
To fill out the ADA Dental Claim Form correctly, every section must be completed unless otherwise directed. Start with the header information to indicate the type of transaction. Fill in the policyholder or subscriber information clearly, ensuring no fields are skipped. If there is other dental or medical coverage, complete sections 4 through 11 as directed. Patient information is crucial, including their relationship to the policyholder and their status. Record all provided services with accurate dates, descriptions, and fees. If the patient has missing teeth, mark this appropriately. Don't forget to sign and date the form where authorizations are required. Lastly, if submitting a claim for secondary insurance, attach the primary insurer's Explanation of Benefits (EOB) and utilize the remarks section if necessary.
Can you submit the ADA Dental Claim Form electronically?
Yes, the ADA Dental Claim Form can be submitted electronically, which is a convenient and efficient method for dental practices. Many insurance companies and dental benefit plans accept electronic submissions, which can speed up the processing time for claims and potentially lead to faster reimbursement. It's advisable to check with the specific insurer for their guidelines on electronic submissions to ensure compliance and proper claim processing.
What should you do if the number of procedures exceeds the space available on the form?
If the number of procedures provided to the patient exceeds the lines available on one ADA Dental Claim Form, the remaining procedures must be listed on a separate, fully completed claim form. Ensure that each form is filled out with consistent patient and policyholder information for continuity and to prevent processing delays. This means each form must be individually complete to stand alone for the insurance company's review.
How do you handle Coordination of Benefits (COB) with the ADA Dental Claim Form?
For Coordination of Benefits (COB), when a claim involves more than one dental insurance plan, you must fill out the ADA Dental Claim Form in its entirety for both insurers. Attach the primary payer's Explanation of Benefits (EOB) to the claim form submitted to the secondary insurer. This shows the amount paid by the primary insurer. The “Remarks” section (Item #35) can be used to indicate the amount paid by the primary carrier and any other pertinent information required by the secondary insurer. This procedure helps streamline the COB process and ensures that all parties have the information needed to process the claim appropriately.
Filling out the ADA Dental Claim Form requires attention to detail, and mistakes can delay processing or result in denied claims. Here are nine common errors:
1. Type of Transaction oversight: Not marking the appropriate box or boxes in section 1 can lead to confusion regarding the purpose of the submission. Whether it's a statement of actual services or a request for predetermination/preauthorization, clear communication from the start ensures the insurance company processes the form as intended.
2. Ignoring Predetermination/Preauthorization Number: If the services require predetermination or preauthorization, failing to include this number (section 2) can significantly delay processing. This number connects the dots for insurance companies, showing that the submitted services have been pre-approved.
3. Incorrect Policyholder Information: Section 12 demands the full name (including middle initial and suffix), address, city, state, and ZIP code of the policyholder/subscriber. Inaccurate or incomplete information here can lead to claim rejections because the insurance company cannot match the claim to an active policy.
4. Forgetting Other Coverage: Neglecting section 4, or incorrectly completing sections 5-11 when another dental or medical coverage is applicable, can mess up the coordination of benefits. This mistake can lead to the primary insurer denying a claim that should have been partially covered by another plan.
5. Misidentifying the Patient's Relationship to the Policyholder: In section 18, the relationship is crucial for determining eligibility and coverage levels. A misstep here can cause outright denial if the insurance company cannot verify the patient as a dependent or spouse.
6. Omission of Student Status: Failure to provide the student status of a dependent (section 19), when applicable, might lead to a denial for services that are only covered for full-time students under certain policies.
7. Procedure-related Fields Incomplete: Sections 24-31, which detail the services provided, are often filled out incorrectly. Each procedure must have a date, description, tooth number (if applicable), and fee. Missing any part of this information can delay claim processing as the insurer seeks clarification or verification.
8. Inaccurate Missing Teeth Information: Section 34 requires an 'X' on each missing tooth. This section is critical for accurate claims related to bridges, dentures, and other services where the current state of the patient's teeth affects coverage. Overlooking or incorrectly marking this section can lead to incorrect benefit calculations.
9. Provider Information Omissions: Sections 48-58 demand comprehensive provider information, including NPI (National Provider Identifier) and if relevant, the Provider Specialty Code (section 56A). Inaccuracies here not only impede direct payment to the provider as authorized in section 37 but may also cause delays if the insurance company can't verify the provider's qualifications or identity.
Avoiding these mistakes requires diligence and a thorough understanding of the ADA Dental Claim Form's requirements. Accurate and complete submissions help ensure timely processing and payment of dental claims.
When dealing with dental care and insurance, the ADA Dental Claim Form becomes a cornerstone for processing and reimbursing claims. However, this form often requires the submission of additional forms and documents to ensure comprehensive and accurate processing. Below is a list of documents that are frequently used alongside the ADA Dental Claim Form.
In addition to the core ADA Dental Claim Form, these documents play pivotal roles in the seamless processing of dental insurance claims. They provide a comprehensive view of the patient's needs, the rationale for treatment, and evidence of procedures performed, ensuring that both the patient and the provider navigate the insurance system effectively.
The ADA Dental Claim form shares similarities with the Medical Claim Form used by medical professionals to submit claims to health insurance companies for reimbursement of services provided. Both forms require detailed patient information, insurance policy details, and a comprehensive record of services provided. They also necessitate the provider's information, including professional identifiers like NPI numbers, and are used to communicate between healthcare providers and insurance entities to facilitate payment for services.
Another document closely related to the ADA Dental Claim form is the Pharmacy Benefit Claim Form, which pharmacies use to request reimbursement from health insurance companies for prescription medications dispensed. Like the dental claim form, it includes patient information, insurance coverage details, and specifics about the service provided—in this case, the medication dispensed. Both forms play a critical role in the billing process within their respective healthcare sectors.
The Health Insurance Claim Form (HCFA-1500) used by physicians and other healthcare providers to claim insurance benefits is also akin to the ADA Dental Claim form. They both collect comprehensive patient and insurance information and itemize the services provided for insurance reimbursement purposes. These forms ensure that providers include necessary details for insurers to process claims efficiently.
The Vision Claim Form used by optometrists and ophthalmologists for billing vision insurance plans bears resemblance to the ADA Dental Claim form as well. Both necessitate detailed information about the patient, the insurance policy, and a record of services provided. They cater to the specific needs of their respective fields but follow a similar structure in collecting and presenting information for insurance claims.
Moreover, the Workers' Compensation Claim Form, utilized when a person is injured at work and requires medical treatment, parallels the ADA Dental Claim form in its purpose of facilitating insurance benefits. They both demand details about the patient and the service provider, alongside specifics of the incident or injury, to support the claim for insurance benefits. The primary difference lies in the nature of the coverage—work-related injuries versus dental services.
The Automobile Insurance Medical Claim Form is another analogous document, designed for situations where medical services are needed due to a car accident. Like the dental claim form, it collects patient demographics, insurance information, and details of the medical services provided. Both forms are integral to the process of claiming insurance benefits for covered services following an incident.
The Disability Insurance Claim Form also shares similarities with the ADA Dental Claim form, particularly in their function of enabling patients to claim insurance benefits. While focused on different types of benefits (disability versus dental), both require detailed information on the claimant, the policy, and the nature of the claim to process and grant insurance benefits.
Finally, the Life Insurance Claim Form, although used in the context of claiming life insurance benefits, has procedural parallels with the ADA Dental Claim form. Both involve submitting detailed information to an insurance company for the purpose of claiming benefits. While the nature of the claim differs significantly, the fundamental process of providing necessary information to support a claim is consistent across both forms.
When completing the ADA Dental Claim form, it is crucial to follow specific do's and don'ts to ensure the form is filled out accurately and efficiently.
These steps will assist in the prompt and accurate processing of dental claims, benefiting both the patient and the dental provider.
Understanding the ADA Dental Claim form is crucial for ensuring the smooth processing of dental insurance claims. However, there are several misconceptions about how to complete and use the form properly. By addressing these misconceptions, policyholders and providers can more effectively manage their submissions and expectations around dental claims.
Misconception 1: All sections of the form must always be completed. While it's important to provide comprehensive information, not all sections are required for every submission. The form is designed to accommodate different types of transactions - such as statements of actual services or requests for preauthorization. Sections relevant to the specific transaction should be completed, as noted in the instructions that accompany the form.
Misconception 2: The ADA Dental Claim Form is only for the patient's current treatment. In addition to information about current treatments, the form also requests details of the patient's insurance coverage and any other relevant financial arrangements. This can include other dental or medical coverage details, ensuring a complete picture of the patient’s benefits and obligations.
Misconception 3: The form doesn't accommodate multiple procedures. If the number of procedures exceeds the space provided on the form, additional procedures should be listed on a separate, fully completed claim form. This ensures that the insurer or another reviewing party has all the necessary information to process the claim efficiently.
Misconception 4: The National Provider Identifier (NPI) and Additional Provider Identifier are the same. The NPI is a unique identifier assigned to providers by the Federal government. In contrast, the Additional Provider Identifier could be a Social Security Number, Tax Identification Number, or a Legacy Identifier, depending on what is used by the billing dentist or dental entity, highlighting a critical distinction in provider identification.
Misconception 5: Information on missing teeth is not important. The section for missing teeth is essential for a comprehensive evaluation of the patient's dental health and history. Placing an 'X' on each missing tooth helps the insurance company or dental benefit plan assess the necessity and relevance of the submitted procedures.
Misconception 6: Provider specialty codes are arbitrary. These codes accurately describe the type of dental professional delivering the treatment, which can influence the approval and payment process. Correctly entering the provider specialty code ensures that the claim is processed in accordance with the specific services rendered.
By clarifying these misconceptions, individuals and providers can navigate the complexities of dental claims with greater confidence and efficiency, ensuring accurate and timely processing of their claims.
When filling out the ADA Dental Claim Form, it's crucial to consider several key takeaways to ensure that the form is complete, accurate, and compliant with the relevant requirements. These insights facilitate a smoother claim process for both patients and dental care providers.
By adhering to these guidelines, you can improve the efficiency and accuracy of the dental claim submission process. It's also beneficial to stay updated with any changes to the form instructions or requirements by checking the ADA’s website regularly.
P&l Statement Template - This document serves as a comprehensive overview of a company's financial performance, evaluating its ability to generate profit.
Roof Certification Template - It is a preemptive measure against future disputes regarding the roof's condition, setting clear expectations for the warranty period.
Act 221 Disclosure - It is a legal requirement in Illinois for sellers to complete this form, aiding in the transparency of the unit's financial and legal standing.