Fill a Valid Annual Physical Examination Form
Fill a Valid Annual Physical Examination Form
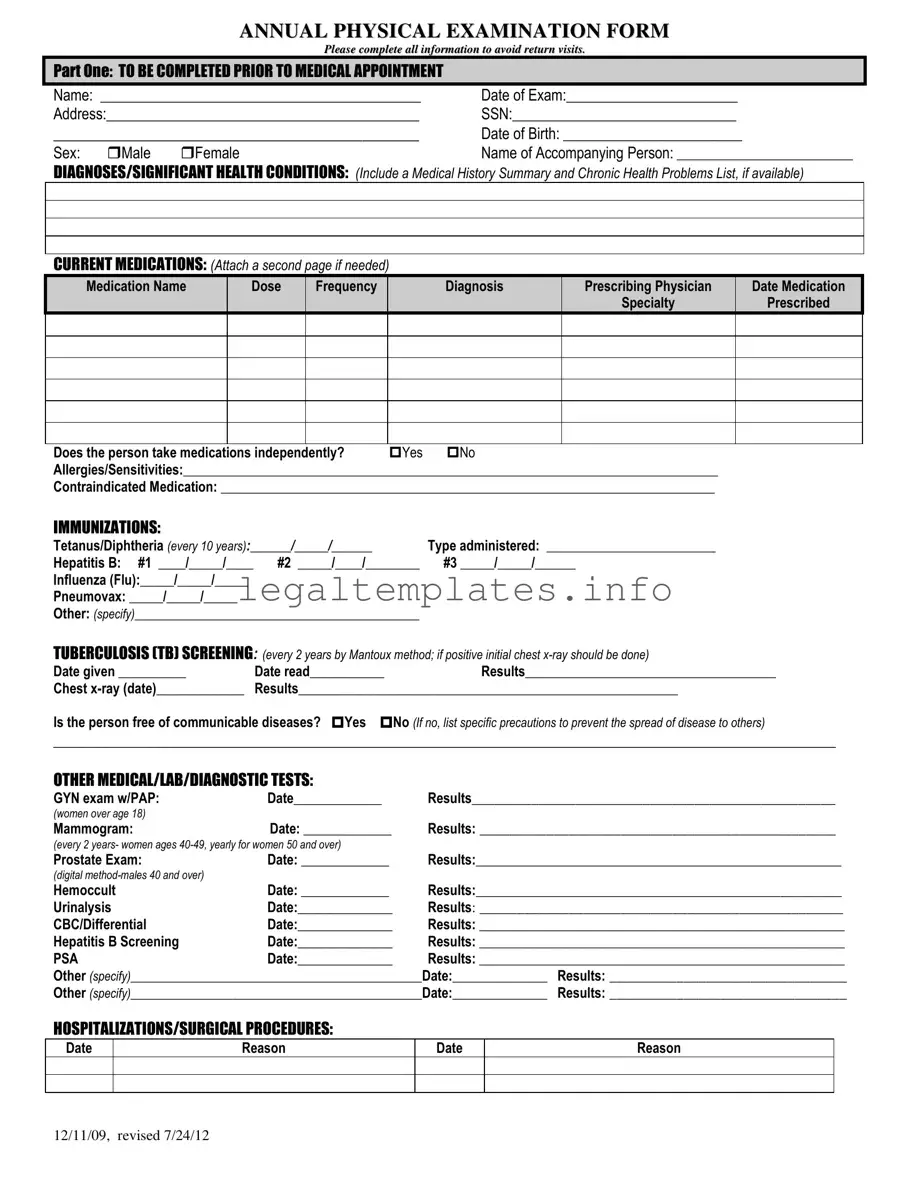
Staying on top of health is paramount, and the Annual Physical Examination form plays a crucial role in this ongoing process. Designed to be thorough, this form ensures individuals and healthcare providers have a comprehensive overview of the patient's health status, medical history, and any specific needs or concerns that might require attention over the next year. At the outset, the form gathers basic yet critical information such as name, date of birth, SSN, and contact data, setting the foundation for a personalized healthcare approach. It delves into critical areas like diagnoses, current medications—detailing the name, dosage, and frequency—immunization records, and screening results for conditions such as tuberculosis. Additionally, it addresses allergies, potential medication contraindications, and the patient's capacity to manage their medication independently, painting a complete picture of the individual's health landscape. Hospitalization and surgical histories are noted, ensuring that the examining physician has a full understanding of past major health events. The form also emphasizes regular screenings such as blood pressure, vision, and hearing, alongside detailed evaluations across various systems of the body—cardiovascular, gastrointestinal, musculoskeletal, to name a few. With prompts for additional comments from healthcare providers, the form is exhaustive, ensuring nothing is overlooked during the physical exam. Furthermore, it concludes with recommendations for maintaining or improving health, including diet, exercise, and any necessary specialist consults, ultimately serving as a vital tool in proactive health management and prevention strategies.
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
| Fact Name | Detail |
|---|---|
| Form Revision Dates | The form was originally issued on 12/11/09 and revised on 7/24/12. |
| Comprehensive Personal Information | Includes detailed sections for personal identification, medical history, medications, allergies, and vaccinations. |
| Systematic Health Screening | Part Two focuses on a general physical examination including vital signs, system evaluations, and screenings for vision and hearing. |
| Follow-Up Care Recommendations | It prompts for recommendations on health maintenance, further specialist evaluations, and modifications to medication or therapy. |
| Governing Law | While the form is generic, the requirement for an annual physical examination may be mandated by state-specific laws governing health and safety regulations in workplaces or schools. |
Filling out an Annual Physical Examination form is a necessary step to ensure all your medical information is accurately recorded for your upcoming appointment. This comprehensive documentation process is crucial for maintaining an up-to-date and detailed medical history. It covers everything from personal information to medical history, current medications, immunizations, and the results of previous screenings and tests. Correctly filling out this form can significantly streamline the appointment process, prevent unnecessary repeat visits, and enable healthcare providers to offer the best care possible. Let's walk through the steps of completing this form.
Once all sections are thoroughly completed, review the form to ensure that no detail is overlooked. Accurate and detailed information plays an integral role in facilitating effective healthcare services. Bringing this form to your annual physical examination will help your healthcare provider offer personalized and comprehensive care, tailored to your current health status and medical history.
What is the purpose of the Annual Physical Examination form?
The purpose of the Annual Physical Examination form is to provide a comprehensive overview of an individual's current health status. It gathers detailed information about the patient's medical history, diagnoses, medications, immunizations, and results from various medical, lab, and diagnostic tests. It aims to identify any health issues early on, track any changes in the patient's health over time, and help in the planning of medical care. Completing this form thoroughly ensures that healthcare providers have all the necessary information to offer the best possible care, and helps to avoid unnecessary return visits.
Why do I need to complete all the information on the form?
Completing all the information on the form is crucial because it provides your healthcare provider with a full picture of your health. This includes your medical history, current medications, immunizations, and recent tests or procedures, among other details. Accurate and comprehensive information helps in making informed decisions about your care, identifying any potential health issues early, and ensuring that your healthcare plan is up-to-date. It also prevents the need for follow-up visits to collect missing information, saving you time and helping to manage your health more efficiently.
Can I attach additional pages if there’s not enough space for my medications?
Yes, you are encouraged to attach additional pages if the space provided for listing your current medications is not sufficient. It's important to include detailed information about each medication, such as the name, dosage, frequency of intake, the diagnosis for which it was prescribed, the prescribing physician, and the date it was prescribed. Providing a complete list of medications, including any over-the-counter drugs or supplements you're taking, ensures that your healthcare provider has a comprehensive understanding of your treatment regimen.
What should I do if I don’t have all the required information for the form?
If you find that you do not have all the required information to complete the form, it's important to gather as much of it as possible before your appointment. You may need to contact previous healthcare providers for records of immunizations, past medical tests, or procedures. If there are sections you cannot complete, inform your current healthcare provider at the time of your appointment. They can help you determine the best course of action, whether it involves setting up follow-up tests or obtaining records from other sources.
Is the Annual Physical Examination form confidential?
Yes, the Annual Physical Examination form, like all medical records, is confidential. The information you provide is protected under patient privacy laws, such as the Health Insurance Portability and Accountability Act (HIPAA) in the United States. This means that your personal and medical information cannot be disclosed to anyone except as necessary for your medical care or as required by law, without your explicit consent.
How often do I need to fill out the Annual Physical Examination form?
The Annual Physical Examination form is intended to be completed once every year. This yearly health checkup helps in monitoring your health over time, identifying any new or potential health issues, and updating your medical care plan accordingly. It is an essential part of preventative healthcare and ensures that you and your healthcare provider are aware of any changes in your health status.
What happens if my health status changes after I've submitted the form?
If your health status changes after you've submitted the form, it's important to inform your healthcare provider as soon as possible. This can include new diagnoses, changes in medication, or other significant health changes. Keeping your healthcare provider informed allows them to offer the most accurate and appropriate care based on your current health needs.
One common mistake people make when filling out the Annual Physical Examination form is not completing all the requested information. This includes leaving fields blank such as the Social Security Number (SSN), Date of Birth, or current medications. The form clearly requests all information to avoid return visits, indicating the importance of providing comprehensive and accurate data for a thorough medical evaluation.
Another error involves inaccuracies in the medication section, particularly with the dosage, frequency, and diagnosis related to the prescribed medication. Some individuals may not accurately recall their medication details or may inadvertently provide outdated information. This can lead to misunderstandings about their health management and potentially impact their care plan.
Incorrect listing of immunization records is also a common oversight. Individuals might forget to update or accurately recall dates and types of vaccinations received, such as for Tetanus/Diphtheria, Hepatitis B, or Influenza. This information is critical for maintaining an up-to-date immunization schedule and ensuring necessary protection against various diseases.
Failure to accurately report personal or family health history, especially regarding diagnoses or significant health conditions, is another frequent mistake. This part of the form is essential for understanding potential hereditary or lifestyle factors that may influence an individual's health. Omitting or incorrectly detailing this information can hinder a comprehensive health assessment.
Many people also neglect to fully detail their allergies or sensitivities, including contraindicated medications. This oversight can have serious implications, as it involves the safety and efficacy of prescribing medication. It is vital to provide a complete and accurate list of all known allergies and contraindicated substances to prevent adverse reactions.
Lastly, failing to update the information regarding hospitalizations, surgical procedures, and diagnostic tests can lead to an incomplete health profile. Events such as recent hospital stays or surgeries, and their reasons, are crucial for the examining physician to understand the current and past health state of the individual, guiding both diagnostic and preventive health measures effectively.
When undergoing an annual physical examination, it's crucial to be thorough to ensure a complete understanding of one's health status. The Annual Physical Examination form is a key document in this process, but it's often just one piece of a larger puzzle. Several other forms and documents usually complement this form to provide a comprehensive overview of a patient's health.
Together, these documents play a vital role in providing healthcare providers with a full picture of a patient's health. They ensure that care is appropriate, up-to-date, and in the best interests of the patient. By maintaining and regularly updating these documents, patients and healthcare providers can work together more effectively to manage health and prevent disease.
The Annual Physical Examination form draws notable parallels to the Medical History form often used by healthcare providers. Both forms play a critical role in collecting comprehensive patient information, including past medical history, chronic health conditions, and a list of current medications. The Medical History form, like the Annual Physical Examination form, requests detailed personal health data to ensure a holistic approach to patient care. It emphasizes the importance of having a complete picture of the patient's health status, including allergies, previous diagnoses, and family medical history, to inform current and future medical decisions and treatments.
Another document closely resembling the Annual Physical Examination form is the Pre-Operative Assessment form. This form focuses on gathering specific health information before surgical procedures. Similar to the annual exam form, it includes sections on patient identification, medical history, current medications, and allergies. The Pre-Operative Assessment is crucial for identifying any potential risks associated with surgery, ensuring the patient's health status is appropriately evaluated and monitored. Like the Annual Physical Examination form, it aims to minimize complications by meticulously reviewing the patient’s health profile prior to surgery.
The Medication Administration Record (MAR) shares similarities with the Annual Physical Examination form’s section on current medications. The MAR is an essential document used in various healthcare settings to record all the medications prescribed to a patient, including the dosage, frequency, and the name of the prescribing physician. This document ensures that medication is administered safely and effectively, tracking the patient's medication regimen over time. Both the MAR and the Annual Physical Examination form underscore the critical role accurate and up-to-date medication information plays in patient care and safety.
The Immunization Record is yet another document akin to the Annual Physical Examination form, particularly in the section detailing a patient's immunization status. This record keeps track of all vaccines a person has received, including the dates and types of vaccines administered. Ensuring that immunization records are current is vital for preventing disease outbreaks and for individual health protection. Similarly, the Annual Physical Examination form collects information on immunizations to assess the patient's preventive care status, demonstrating the shared objective of both documents to maintain a comprehensive overview of the patient’s preventive health measures.
Lastly, the Emergency Medical Information form echoes parts of the Annual Physical Examination form, especially in conveying critical health information that could affect emergency treatment. This document often includes details about chronic conditions, allergies, medications, and contact information for primary care providers, mirroring the comprehensive health overview provided by the annual physical form. Both documents serve as vital tools for informing healthcare decisions, especially in urgent situations where understanding a patient's existing health issues and treatment preferences is immediately necessary.
When filling out the Annual Physical Examination form, it is important to follow these guidelines to ensure accurate and complete medical information is provided. Here are ten do's and don'ts to keep in mind:
Adhering to these guidelines can help ensure that your annual physical examination form is filled out correctly, which can subsequently facilitate better healthcare outcomes.
When it comes to an Annual Physical Examination Form, there are a handful of misconceptions that can lead to confusion. Let's clear the air about some of these common misunderstandings:
Understanding these points can demystify the process of completing the Annual Physical Examination Form and highlight its importance in maintaining your health. Remember, this document is a tool for you and your healthcare provider to keep track of your health status and needs over time.
Filling out an Annual Physical Examination form is crucial for maintaining your health. Here are five key takeaways to remember when completing this form and using the information it gathers:
Overall, the Annual Physical Examination form is essential for tracking your health status, maintaining preventive care, and ensuring the proper management of existing conditions. It's a tool that not only guides your health care provider in offering the best care possible but also involves you actively in the care process.
How to Create Payroll Checks - A wage statement from an employer detailing the amount paid to an employee and all pertinent deductions.
Dnd Form Fillable Character Sheet - Character sheets detail the achievements and failures of a character, reflecting their journey and growth.