Fill a Valid DD 2870 Form
Fill a Valid DD 2870 Form
Navigating the complexities of medical records and their disclosure can sometimes feel overwhelming. Central to this process for military personnel and their families is the DD 2870 form, Authorization for Disclosure of Medical or Dental Information. This form plays a pivotal role in ensuring that medical or dental records are shared securely and with consent, respecting patients' privacy and confidentiality. Whether it's about transferring records between facilities, providing information to insurance companies, or enabling family members to assist with medical care, the DD 2870 simplifies the authorization process. Its careful completion guarantees that only the specified data requested by the individual, or their legal representative, is disclosed, and only to those entities they have approved. Understanding this form’s function, how to fill it out correctly, and recognizing the situations in which it is necessary can significantly streamline the often intricate health information management practices within the military healthcare system.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
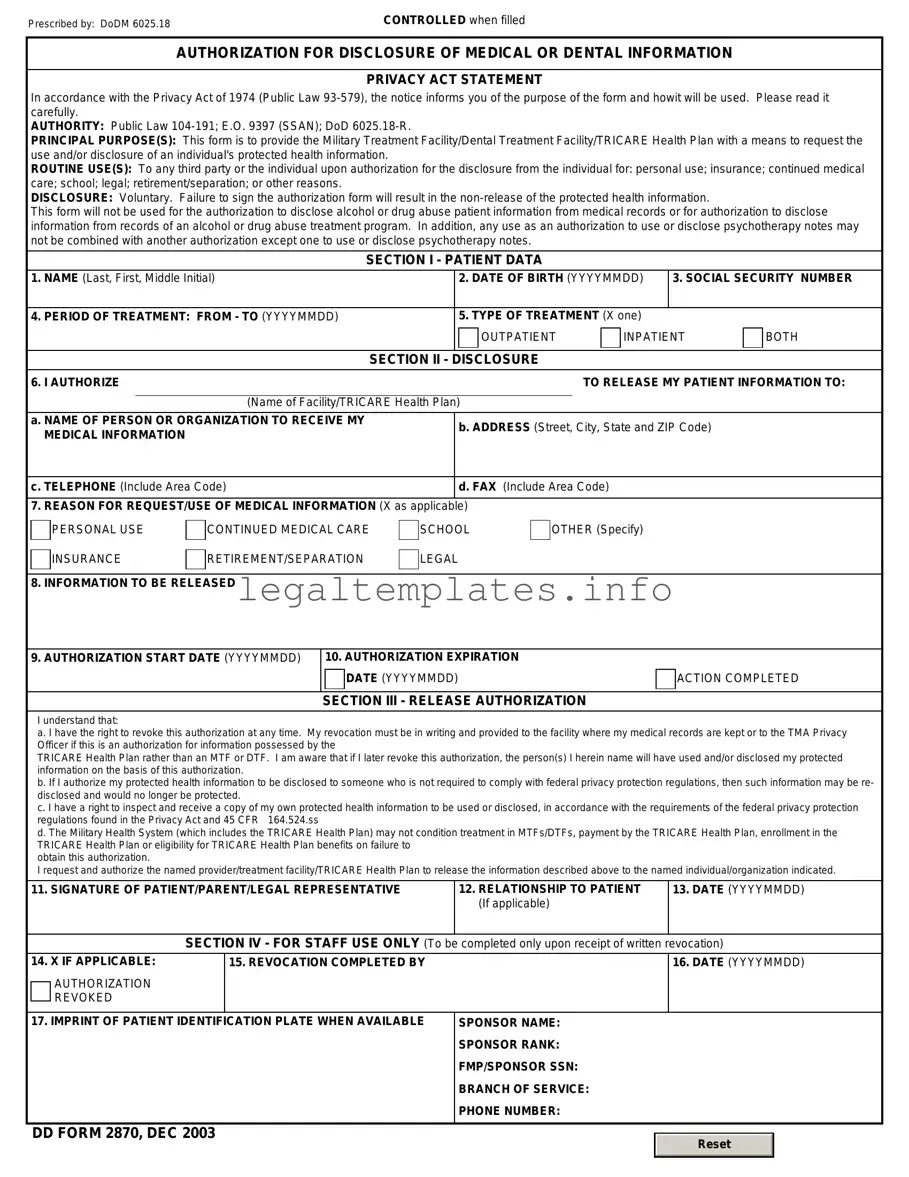
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
| Fact Number | Description |
|---|---|
| 1 | The DD 2870 form is used to authorize disclosure of medical or dental information. |
| 2 | It is typically utilized within military healthcare systems, such as the Department of Defense (DoD) or TRICARE. |
| 3 | The form requires information about the patient, the type of records to be disclosed, and the purpose of the disclosure. |
| 4 | Individuals can specify restrictions regarding the extent of the information shared through the form. |
| 5 | A valid DD 2870 form must be signed by the patient, or a legal representative if the patient is a minor or unable to consent. |
| 6 | The authorization is typically valid for one year, after which a new form must be completed for continued information sharing. |
| 7 | It serves as a legal document ensuring that medical information is shared in compliance with the Health Insurance Portability and Accountability Act (HIPAA). |
| 8 | The form can be revoked by the patient at any time, which would stop any future sharing of information as specified. |
| 9 | While the DD 2870 is a federal form, its implementation and adherence to HIPAA are consistent across all states, without state-specific versions. |
Completing the DD 2870 form is a crucial process for individuals seeking to authorize the disclosure of their medical or dental information. The precise completion of this form is essential to facilitate the seamless sharing of pertinent information between parties, ensuring that your healthcare or dental records can be accessed by those you designate. This step-by-step guide outlines the necessary steps to accurately fill out the form, thereby avoiding any potential delays or issues in the processing of your request.
Upon completion of the DD 2870 form, review all sections thoroughly to ensure the accuracy of the information provided. Incorrect or missing information may result in delays. Once the form is accurately filled and signed, proceed to submit it to the appropriate office or individual specified in the instructions accompanying the form. Prompt submission will aid in the timely processing of your request.
What is a DD 2870 form used for?
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is used to grant permission for the release of an individual's medical or dental records to authorized recipients. This form is often utilized within the Department of Defense (DoD) and related healthcare settings, serving as a formal way to ensure patient consent is obtained before sharing sensitive health information with other parties, such as insurance companies, healthcare providers, or legal representatives.
Who needs to fill out the DD 2870 form?
Any individual who wishes to have their medical or dental records released or shared with a third party must fill out the DD 2870 form. This requirement applies to service members, dependents, retirees, and other beneficiaries who receive care within the Military Health System. It ensures that the patient's privacy is protected, and their records are only shared with their consent.
Where can I obtain a DD 2870 form?
The DD 2870 form can be obtained from any medical treatment facility (MTF) within the Department of Defense, including hospitals and clinics. Additionally, it is available online through various DoD websites and portals that provide access to military forms. Patients can also request the form from healthcare providers or administrative offices within their healthcare network.
How is the DD 2870 form submitted?
After filling out the DD 2870 form, it should be submitted directly to the medical treatment facility (MTF) where the patient receives care or where their records are held. Submission can typically be done in person, by mail, or through secure electronic methods, depending on the facility's protocols. It is essential to follow the specific instructions provided by the healthcare provider or MTF to ensure proper handling and privacy compliance.
What information is needed to complete the DD 2870 form?
To complete the DD 2870 form, individuals must provide personal identification information, including their name, date of birth, and Social Security Number (SSN) or DoD Identification (ID) number. The form also requires specific details about the information being requested, such as the type of records, the dates of service concerned, and the purpose of the disclosure. Additionally, the name and address of the recipient(s) authorized to receive the information must be clearly stated.
Is there a deadline for submitting the DD 2870 form?
While there is no universal deadline for submitting the DD 2870 form, timely submission is crucial to avoid delays in the processing of requests for medical or dental records. It is advisable to submit the form well in advance of when the records are needed, especially if they are required for time-sensitive matters such as claims processing, legal cases, or continuity of care. The specific healthcare provider or facility may provide guidance on their processing times.
Can I revoke the authorization provided on the DD 2870 form?
Yes, the authorization granted through the DD 2870 form can be revoked by the individual who originally provided it. To do so, the individual must submit a written statement to the same medical treatment facility (MTF) where the original authorization was sent, indicating their desire to revoke the consent. This statement effectively nullifies the authorization and stops any further sharing of the individual’s health information based on the previously submitted form.
What if my request for information via the DD 2870 form is denied?
If a request for information based on the DD 2870 form is denied, the individual has several options. Firstly, it is important to understand the reason for the denial, which should be provided by the facility or entity handling the request. Common reasons may include incomplete information on the form or a failure to prove the necessity of the disclosure. Depending on the reason, the individual may be able to correct any errors and resubmit the form or appeal the decision through channels specified by the medical treatment facility or healthcare provider.
Filling out the DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, is a task that requires attention to detail. A common mistake people make is not checking for completeness. Often, individuals overlook certain fields or sections, assuming they may not be applicable to their situation. This oversight can lead to incomplete forms, resulting in the delay or denial of the request for information. It’s crucial to review each section carefully and fill out all necessary information to avoid such issues.
Another area where errors frequently occur is in the specification of information to be disclosed. People sometimes fail to clearly identify the specific type of medical or dental records they need. This lack of specificity can lead to the release of more information than intended or, conversely, not enough information. Being precise about the dates of service, types of records, and purpose for the request can streamline the process and ensure the correct information is disclosed.
Incorrect or outdated personal information is another common mistake. When filling out the DD 2870 form, it's important to provide current and accurate personal information. This includes the social security number, military rank, and contact information. Any discrepancies between the information provided and official records can complicate the identification process and delay the release of medical or dental information. Ensuring accuracy in this area is critical for a smooth process.
Many individuals forget to include the necessary signatures on the form. The DD 2870 requires signatures from both the requestor and the individual whose records are being requested, if they are not the same person. Missing signatures can invalidate the entire request, requiring the form to be resubmitted. This oversight can significantly delay the retrieval of needed information, emphasizing the importance of double-checking the form before submission.
Lastly, a failure to specify the method of disclosure is a mistake that can lead to confusion and further delays. The form allows for different methods of disclosure, such as fax, mail, or electronic delivery. Without clear instructions on how the information should be sent, processing the request can become more complicated, potentially leading to the mishandling of sensitive information. Indicating the preferred method of disclosure ensures that the records are transmitted in a manner that meets the requester’s needs and secures the information properly.
Completing the DD 2870 form, which authorizes the disclosure of medical or dental information, often requires additional documentation to ensure proper handling and compliance with regulatory standards. When managing healthcare information, especially within military communities, a comprehensive approach is necessary. The forms and documents that typically accompany the DD 2870 help streamline processes, ensuring that all necessary permissions are in place and that information is shared securely and effectively.
Together, these documents facilitate a thorough and legally compliant approach to the handling of sensitive information. They ensure that the individual's rights and wishes are respected and that all parties involved are adequately informed and authorized to make or act upon health-related decisions. Understanding and preparing these additional forms can significantly enhance the effectiveness and efficiency of the medical information disclosure process.
The DD 2870 form, Authorization for Disclosure of Medical or Dental Information, shares similarities with the HIPAA Authorization Form. Both documents allow individuals to grant permission for the disclosure of their personal health information. These forms ensure that sensitive health details are shared in compliance with privacy laws, specifically protecting the individual's health information. The HIPAA Authorization Form, like the DD 2870, requires the individual's signature to authorize the release of medical records, ensuring the control over who can access this information remains with the patient.
Comparable to the DD 2870 is the Release of Information form often used in non-military healthcare settings. This document also facilitates the process of sharing an individual’s medical or dental information between healthcare providers or with third parties, like insurance companies. It necessitates explicit consent from the patient before any information is disclosed, mirroring the DD 2870’s requirement for patient authorization. These forms play a critical role in maintaining patient confidentiality while allowing necessary medical information exchange.
The Power of Attorney (POA) for Healthcare is another document that parallels the DD 2870 in granting someone authority over personal matters. However, the POA for Healthcare typically grants broader powers, including decision-making in various medical situations when the individual is unable to do so. Like the DD 2870, it reflects the importance of respecting individuals' preferences and rights concerning their health information and care, ensuring that these decisions are made according to their wishes by a trusted individual.
Lastly, the Consent to Treat form found in many healthcare settings shares the essence of the DD 2870 by requiring a patient's or guardian’s authorization for medical treatment. However, it’s more narrowly focused on permission for medical procedures or interventions rather than the broader authorization for sharing information as in the DD 2870. Nonetheless, both documents underscore the need for informed consent in healthcare, championing the patient's autonomy over their medical care and personal health information.
The DD 2870 form, also known as the Authorization for Disclosure of Medical or Dental Information, plays a critical role in managing one's healthcare records. It is instrumental in ensuring that your medical or dental information is shared correctly and with your consent. To navigate this process effectively, there are several dos and don'ts to keep in mind:
Correctly completing the DD 2870 form is essential for the timely and accurate handling of your healthcare information. Following these guidelines will help streamline the process, ensuring your healthcare needs are handled with the care and precision they deserve.
The DD 2870 form, often involved in the process of authorizing disclosure of medical or dental information, is shrouded in misconceptions. Understanding these incorrect beliefs is crucial for anyone trying to navigate through or facilitate the process of information exchange in healthcare settings, especially within military environments.
It Can Be Used for Any Type of Information Request: A common misconception is that the DD 2870 form is a catch-all for any type of information request within the Department of Defense. In truth, it's specifically designed for authorizing the release of medical or dental records, not for other types of information or records requests.
It Allows for Indefinite Access: Some believe once consent is given via the DD 2870 form, it grants indefinite access to one's medical records. However, the form requires specifying the period of authorization, limiting access to a defined timeframe.
Anyone Can File It: The idea that any individual can file a DD 2870 form on someone else's behalf is incorrect. Only the patient or their legal representative has the authority to authorize the release of health information.
It's Only for Military Personnel: Although predominantly used within military settings, the DD 2870 form is also applicable to civilians who receive care at military healthcare facilities. It is not exclusive to military personnel.
No Revocation is Possible: Another misunderstanding is that once signed, the DD 2870 form cannot be revoked. Patients have the right to revoke their consent at any time, although they must do so in writing.
Electronic Signatures Are Not Acceptable: With advancements in digital processing, there's a misconception that the DD 2870 must be signed in ink. In reality, electronic signatures are increasingly accepted, provided they meet the prevailing standards and regulations.
It Guarantees Immediate Access: Submitting a DD 2870 form does not guarantee immediate access to records. The processing time can vary based on the complexity of the request and the workload of the medical records department.
Clarifying these misconceptions is key to ensuring that individuals seeking to authorize the disclosure of medical or dental records have accurate expectations and can navigate the process more effectively.
The DD 2870 form, or Authorization for Disclosure of Medical or Dental Information, is a critical document for many individuals, particularly those associated with the military. It serves as a formal request to disclose medical or dental records to designated recipients. Understanding how to fill out and use this form properly is essential for the smooth processing of such requests. Here are key takeaways to guide you through this process:
Properly filling out and submitting the DD 2870 form plays a crucial role in the timely and accurate transfer of medical or dental information. Whether you're moving to a new duty station, processing a claim, or coordinating care among providers, these takeaways can help streamline the process. Always keep a copy of the filled-out form for your records and follow up if you do not receive confirmation of your request within a reasonable timeframe.
Can I Opt Out of Medicare Part B - Formalizes the decision of a Medicare beneficiary to stop Part B coverage.
Oglala Sioux Tribe Enrollment - The application process is governed by Ordinance 10-26, adopted by the Oglala Sioux Tribal Council.