Fill a Valid Leap application IML-4 Form
Fill a Valid Leap application IML-4 Form
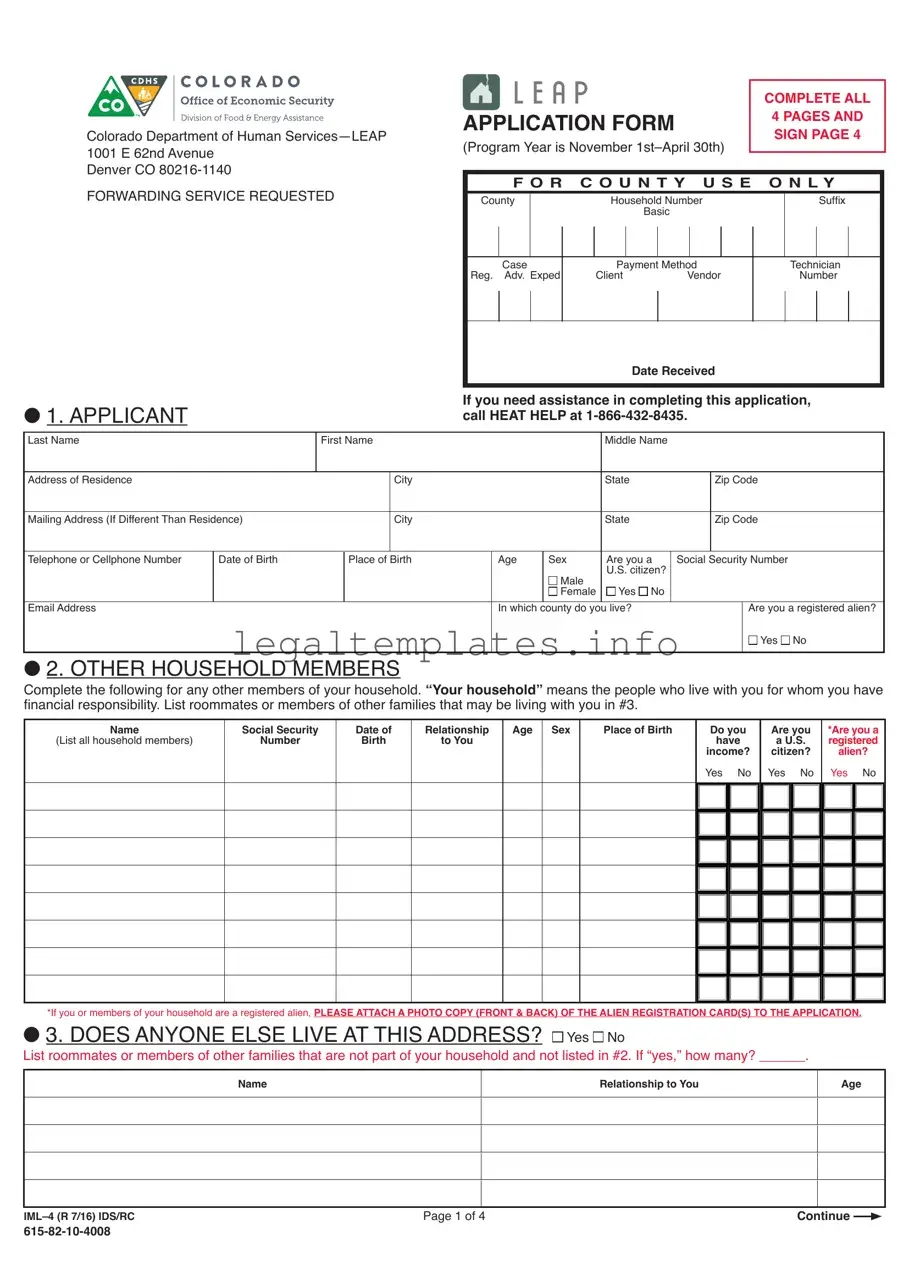
Navigating the intricacies of legal documents and applications can be a daunting task for many individuals. Among these, the Leap application IML-4 form stands out as a crucial document for a specific set of legal processes. Broadly, this form serves as a vital component in applications concerning certain legal matters, though the specific details and requirements can vary significantly depending on the context in which it is used. The importance of accurately completing and submitting the IML-4 form cannot be overstated, as it often plays a pivotal role in the success of the application process it supports. This introduction aims to shed light on the major aspects of the Leap IML-4 form, including its purpose, the typical scenarios requiring its submission, and the general procedures for its completion and filing. While the contents of the form itself are comprehensive, understanding its significance and the correct approach to tackling its requirements is essential for individuals looking to navigate their legal journey efficiently.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMPLETE ALL |
||||
|
|
APPLICATION FORM |
|
4 PAGES AND |
|||||||||||
|
|
||||||||||||||
Colorado Department of Human |
|
SIGN PAGE 4 |
|||||||||||||
(Program Year is November |
|
||||||||||||||
1001 E 62nd Avenue |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Denver CO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
)25:$5',1*6(59,&(5(48(67(' |
|
F O R C O U N T Y U S E O N L Y |
|
||||||||||||
&RXQW\ |
|
+RXVHKROG1XP HU |
|
|
|
6XIÀ[ |
|
||||||||
|
|
|
|
|
|
Basic |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Case |
Payment Method |
|
|
Technician |
|
|||||||
|
|
5HJ $GY ([SHG |
&OLHQW |
|
9HQGRU |
|
|
1XP HU |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Received |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O1. APPLICANT
If you need assistance in completing this application, call HEAT HELP at
Last Name |
|
First Name |
|
|
Middle Name |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Address of Residence |
|
|
|
City |
|
|
State |
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address (If Different Than Residence) |
|
|
City |
|
|
State |
|
|
Zip Code |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
7HOHSKRQHRU&HOOSKRQH1XP HU |
' WHRI%LUWK |
|
3O FHRI%LUWK |
$JH |
6H[ |
$UH\RX |
6RFL O6HFXULW\1XP |
HU |
||||
|
|
|
|
|
|
|
U.S. citizen? |
|
|
|||
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
Female |
Yes |
No |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Email Address |
|
|
|
|
In which county do you live? |
|
|
|
Are you a registered alien? |
|||
|
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
O 2. OTHER HOUSEHOLD MEMBERS
Complete the following for any other members of your household. “Your household” means the people who live with you for whom you have
ÀQ QFL OUHVSRQVL LOLW\ LVWURRPP WHVRUPHP HUVRIRWKHUI PLOLHVWK WP \ HOLYLQJZLWK\RXLQ
Name
(List all household members)
Social Security
Number
Date of
Birth
Relationship
to You
Age
Sex
Place of Birth
Do you |
Are you |
have |
a U.S. |
income? |
citizen? |
Yes No |
Yes No |
|
|
*Are you a registered alien?
Yes No
*If you or members of your household are a registered alien, PLEASE ATTACH A PHOTO COPY (FRONT & BACK) OF THE ALIEN REGISTRATION CARD(S) TO THE APPLICATION.
O '2(6$1<21(( 6( ,9($77+,6$''5(66  Yes
Yes 
 No
No
LVWURRPP WHVRUPHP HUVRIRWKHUI PLOLHVWK W UHQRWS UWRI\RXUKRXVHKROG QGQRWOLVWHGLQ ,I´\HVµKRZP Q\ |
Name
Relationship to You
Age
Page 1 of 4 |
Continue |
|
|
|
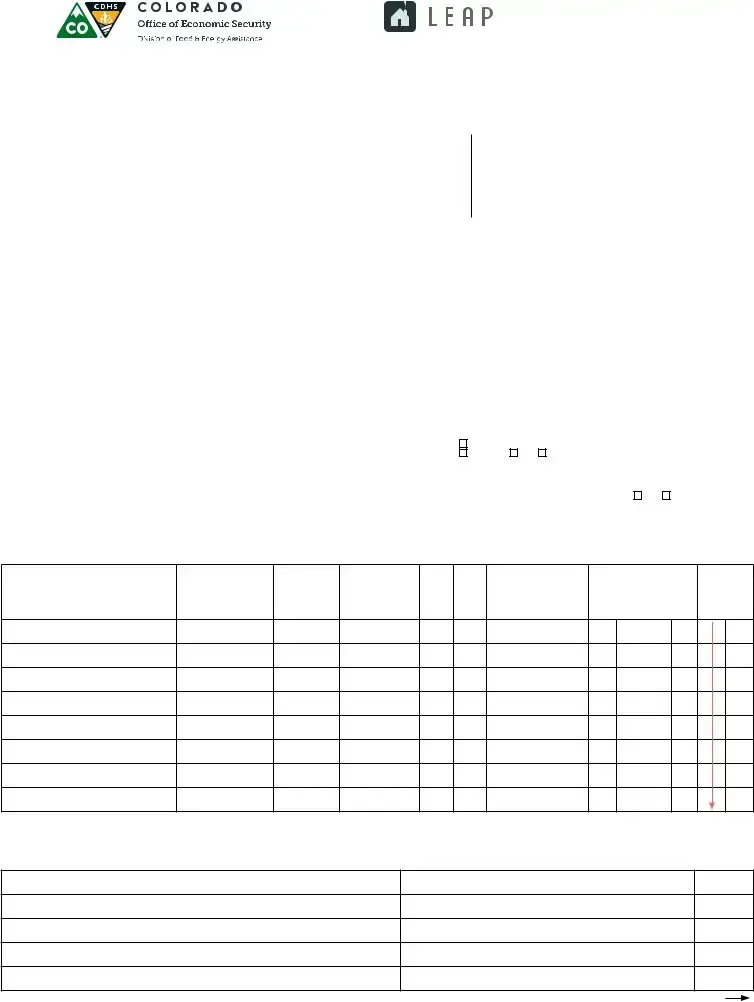
O 4. HOUSEHOLD INCOME
 Does anyone in your household have work income?
Does anyone in your household have work income?  Yes
Yes  No
No
Who Receives It?
How Often Paid?
Gross Monthly
Amount
Employer Name
Initial this box that you have attached copies of pay stubs for at least the 4 weeks prior to the date of application
 Does anyone in your household have
Does anyone in your household have  Yes
Yes 
 No
No
Who Receives It?
How Often Paid?
Gross Monthly
Amount
Employer Name
Initial this box that you
have attached copies of VHOIHPSOR\PHQWSUR W and loss statement for the
month previous to your date
of application
 Does anyone in your household have
Does anyone in your household have  Yes
Yes  No
No
Social Security income (SSA); Supplemental Security Income (SSI); Supplemental Security Disability Income (SSDI); Colorado Works (TANF);
2OG$JH3HQVLRQ2$3$LGWRWKH1HHG\'LV OHG$1'FKLOGVXSSRUW OLPRQ\VSRXV OP LQWHQ QFHYHWHU Q·VGLV LOLW\8QHPSOR\PHQW &RPSHQV WLRQ HQHÀWV:RUNHUV&RPSHQV WLRQGLV LOLW\RUVLFN HQHÀWVSHQVLRQVRUUHWLUHPHQWLQFRPH Q\RWKHULQFRPHSOH VHGHVFUL H
Who Receives It?
How Often Paid?
Gross Monthly
Amount
Type of
as Listed Above
Initial this box that you have attached copies of award letters for the month previous to your date
of application
 'LG\RXS \\RXUH[SHQVHV \ OR QO VWPRQWKRU JLIWIURP IULHQGRUUHO WLYH ,I OR QZK WG WHGLG\RXUHFHLYHWKHPRQH\
'LG\RXS \\RXUH[SHQVHV \ OR QO VWPRQWKRU JLIWIURP IULHQGRUUHO WLYH ,I OR QZK WG WHGLG\RXUHFHLYHWKHPRQH\
Yes  No If Yes, provide a loan repayment schedule. +RZPXFKLVWKHWRW OOR Q
No If Yes, provide a loan repayment schedule. +RZPXFKLVWKHWRW OOR Q
:K WG WHGR\RX HJLQUHS \LQJWKHOR Q |
+RZPXFKPRQH\SHUPRQWK |
,I JLIWVIURP IULHQGRUUHO WLYHZK WG WHGLG\RXUHFHLYHWKHPRQH\ |
+RZPXFKZ VWKHJLIW |
 How did you pay for these following costs if your household income does not cover your basic living expenses?
How did you pay for these following costs if your household income does not cover your basic living expenses?
Rent: |
Food: |
Utilities: |
Other: |
O ,9,1*$55$1*(0(176
Check ( ) the item that best describes the dwelling where you currently live and are applying for assistance.
House/Modular Home |
Rooming/Boarding House |
Fraternity or Sorority House |
Cabin |
'XSOH[7ULSOH[)RXUSOH[ |
Hotel/Motel |
Rehabilitation Center |
Camper |
Townhouse |
& U9 Q%XV |
Correctional Facility |
5th Wheel |
Apartment/Condominium |
Group Home |
Nursing Home/Residential Care Facility |
59 |
Mobile Home |
Dormitory |
2WKHU'ZHOOLQJ3OH VH6SHFLI\ |
|
Do you rent? <HV,I\HVZK |
WLV\RXUPRQWKO\UHQW |
|
|
Do you have a mortgage payment? Yes.
,I\HVZK WLVWKHPRQWKO\PRUWJ JHS \PHQW RUGR\RXRZQ\RXUGZHOOLQJRXWULJKW  Yes Do you pay a lot or space rental amount?
Yes Do you pay a lot or space rental amount?  <HV,I\HVZK WLV\RXUPRQWKO\VS FHUHQWS \PHQW
<HV,I\HVZK WLV\RXUPRQWKO\VS FHUHQWS \PHQW
What is the name and phone number of your apartment complex?
O 6. SUBSIDIZED HOUSING
Do you live in Section 8, public housing, or do you receive a subsidy to pay your rent?  Yes
Yes  No
No
Page 2 of 4 |
Continue |
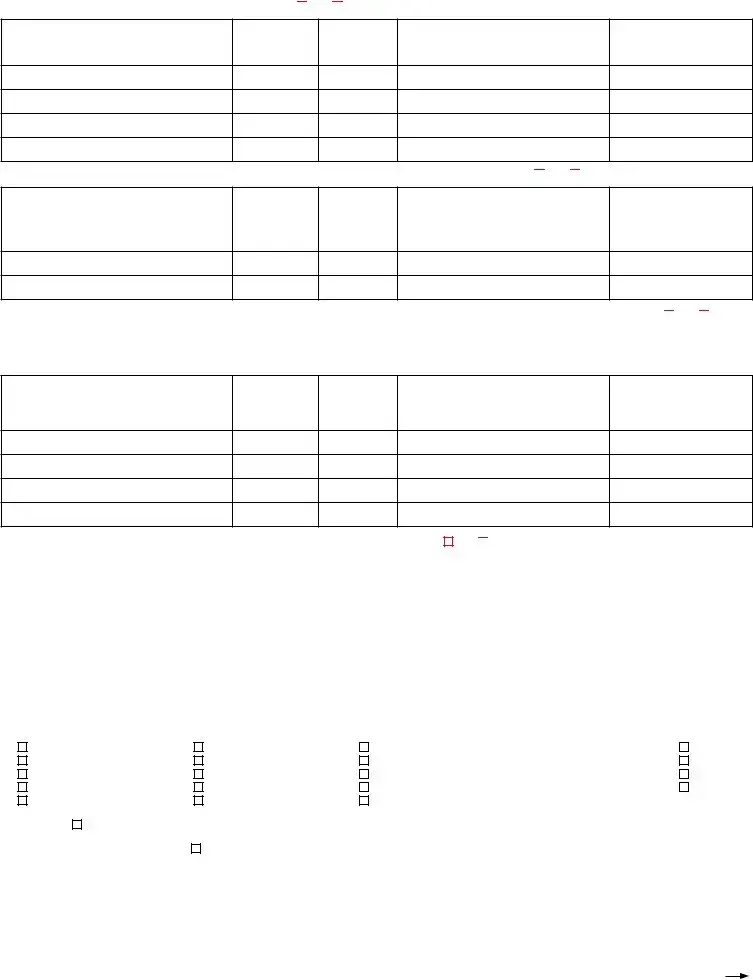
O 7. HEAT/RENT INFORMATION
ARE YOU HAVING AN EMERGENCY WITH YOUR PRIMARY HEATING FUEL RIGHT NOW?  Yes
Yes
If yes, check type of emergency below and attach a copy of the notice from your energy provider:

 $OUH G\GLVFRQQHFWHG'LVFRQQHFW' WH
$OUH G\GLVFRQQHFWHG'LVFRQQHFW' WH

 5HFHLYHGGLVFRQQHFWQRWLFH XWQRW\HWGLVFRQQHFWHG' WHGLVFRQQHFWVFKHGXOHG
5HFHLYHGGLVFRQQHFWQRWLFH XWQRW\HWGLVFRQQHFWHG' WHGLVFRQQHFWVFKHGXOHG
 3URS QHW QNHPSW\RU UH\RXRXWRI XONIXHOVXFK VZRRGIXHORLOHWF $PRXQWQHHGHGIRUPLQLPXPGHOLYHU\
3URS QHW QNHPSW\RU UH\RXRXWRI XONIXHOVXFK VZRRGIXHORLOHWF $PRXQWQHHGHGIRUPLQLPXPGHOLYHU\ 
 3URS QHW QN WRU HORZ$PRXQWQHHGHGIRUPLQLPXPGHOLYHU\
3URS QHW QN WRU HORZ$PRXQWQHHGHGIRUPLQLPXPGHOLYHU\
Check ( ) the main fuel used to heat (not light) your residence. CHECK ONLY ONE.
 Natural Gas
Natural Gas  Propane
Propane  Electricity
Electricity  Wood
Wood  Coal
Coal  Fuel Oil
Fuel Oil  Kerosene
Kerosene  Other: ($3FDQQRWDVVLVWRUSURYLGHDEHQH WIRUDQ\W\SHRISRUWDEOHKHDWLQJV\VWHPV
Other: ($3FDQQRWDVVLVWRUSURYLGHDEHQH WIRUDQ\W\SHRISRUWDEOHKHDWLQJV\VWHPV
Check ( ) the way in which the heat (not light) is paid for at your residence.

 I pay heating costs directly to a utility company or fuel dealer. (If so, attach copy of most recent heating bill).
I pay heating costs directly to a utility company or fuel dealer. (If so, attach copy of most recent heating bill).
1 PHRIIXHOSURYLGHU |
%LOOLQJ FFRXQWQXP HU |
If your electricity is supplied by a different company, please provide:
(OHFWULFFRPS Q\Q PH |
|
$FFRXQWQXP HU |
,I\RXUKH W LOOLVLQVRPHRQHHOVH·VQ |
PHSURYLGHQ PH QG |
GGUHVVRIWK WSHUVRQ QGWKHLUUHO WLRQVKLSWR\RX |
1 PH |
$GGUHVV |
5HO WLRQVKLS |
([SO LQZK\\RXUKH W LOOLVLQWKHLUQ |
PH |
|

 Heat is included in my rent. (If so, attach a copy of the most recent rent receipt that already shows heat is included.)
Heat is included in my rent. (If so, attach a copy of the most recent rent receipt that already shows heat is included.)

 Someone other than a member of my household pays my heating costs.
Someone other than a member of my household pays my heating costs.
Provide name and address of that person and their relationship to you.
1 PH |
$GGUHVV |
5HO WLRQVKLS |
([SO LQZK\WKH\S \\RXUKH W |
LOO |
|
O9(5,),&$7,212) $:)8 35(6(1&(
State law requires applicants for LEAP to provide additional documents with each LEAP application. A READABLE COPY of one of the following VALIDLGHQWLÀF WLRQVPXVW HSURYLGHG
$&RORU GR'ULYHU LFHQVHRU &RORU GR,GHQWLÀF WLRQ& UGRU $8QLWHG6W WHVPLOLW U\F UGRUPLOLW U\GHSHQG QW·VF UGRU
3.A United States Merchant Mariner card; or,
4.A Native American Tribal document.
5.Any other document authorized by rules adopted by the Colorado Department of Revenue (DOR).
IN ADDITION: 7KH SSOLF QWIRU ($3PXVW OVRFRUUHFWO\FRPSOHWHVLJQ QGG WHWKH$IÀG YLWORF WHG HORZ
For more information regarding Lawful Presence law and requirement please go to the DOR web site at: http://www.colorado.gov/revenue.
AFFIDAVIT
for the Colorado Department of Human Services and the Department of Health Care Policy and Financing as Proof of Lawful Presence in the United States
,
Check{
 only one
only one
box
VZH URU IÀUPXQGHUSHQ OW\RIRUSHUMXU\XQGHUWKHO ZVRIWKH6W WHRI&RORU GRWK W
I am a United States citizen, or
I am a legal Permanent Resident of the United States, or
I am lawfully present in the United States pursuant to federal law.
,XQGHUVW QGWK WWKLVVZRUQVW WHPHQWLVUHTXLUHG \O Z HF XVH,K YH SSOLHGIRU SX OLF HQHÀW,XQGHUVW QGWK WVW WHO ZUHTXLUHVPHWRSURYLGH SURRIWK W, PO ZIXOO\SUHVHQWLQWKH8QLWHG6W WHVSULRUWRUHFHLSWRIWKLVSX OLF HQHÀW,IXUWKHU FNQRZOHGJHWK WP NLQJ I OVHÀFWLWLRXVRUIU XGXOHQW
VW WHPHQWRUUHSUHVHQW WLRQLQWKLVVZRUQ IÀG YLWLVSXQLVK OHXQGHUWKHFULPLQ OO ZVRI&RORU GR VSHUMXU\LQWKHVHFRQGGHJUHHXQGHU&RORU GR5HYLVHG 6W WXWH QGLWVK OOFRQVWLWXWH VHS U WHFULPLQ ORIIHQVHH FKWLPH SX OLF HQHÀWLVIU XGXOHQWO\UHFHLYHG
_________________________________________________________________________________ |
_______________________________________________________ |
Signature |
Date |
Page 3 of 4 |
Continue |
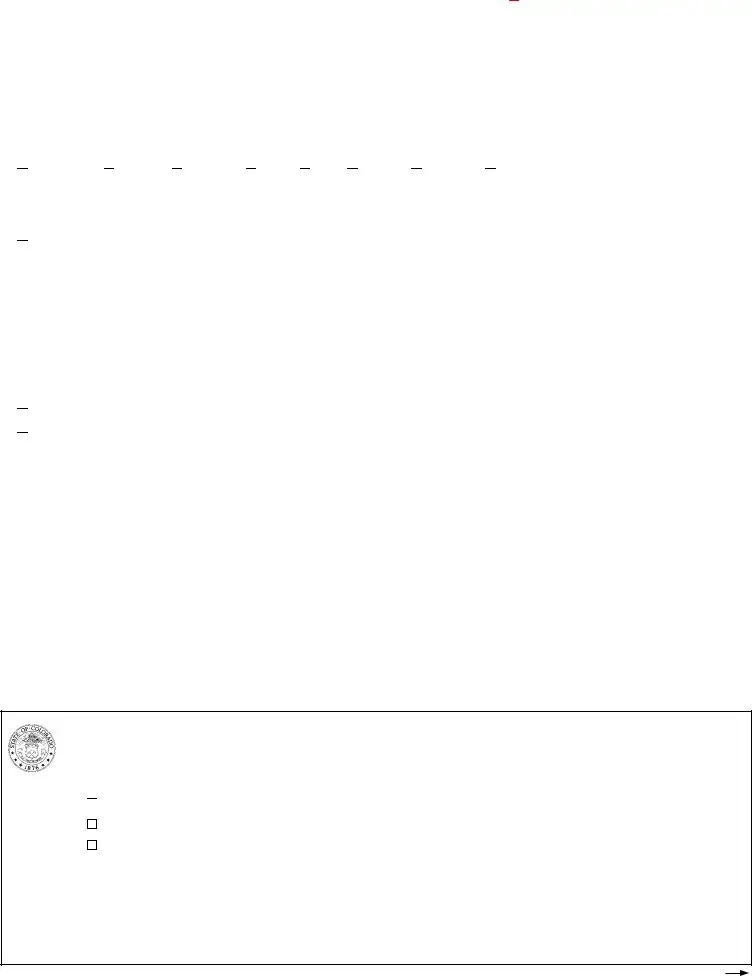
O 9. ADDITIONAL INFORMATION
Information reported in this section will not be used to determine your eligibility for LEAP or your payment level. This information will only be used for statistical information.
Check ( ) here if any member of your household is: 
 Handicapped or disabled
Handicapped or disabled
Race of applicant: Hispanic White Black or African American American Indian or Alaska Native Asian

 1 WLYH+ Z LL QRU2WKHU3 FLÀF,VO QGHU
1 WLYH+ Z LL QRU2WKHU3 FLÀF,VO QGHU Other
Other
I learned about LEAP from the following source (check only one):
Friend |
Senior Center |
6RFL O6HUYLFHV2IÀFH |
|
LEAP Poster |
Newspaper |
Billboard |
PEAK Website |
Heating Company |
Radio |
Bus Benches |
Other |
Received Application in Mail |
LEAP Website |
Television |
|
O 10. CONSENT TO DISCLOSE CUSTOMER DATA
7KH&RORU GR ($3RIÀFH1 Heat Help Line: (866)
SOH VHUHIHUWRWKH ($3ZH VLWHIRU OLVWRI IÀOL WHG JHQFLHVWK WP \SURYLGH\RXZLWK VVLVW QFHZZZFRORU GRJRYFGKV ($3 LVUHTXHVWLQJWK W\RX XWKRUL]H\RXUXWLOLW\VHUYLFHSURYLGHUWRGLVFORVHWKHIROORZLQJLQIRUP WLRQWRWKH ($3RIÀFH
•Your utility account payment history and other account details, such as utility charges, payment history, past due amounts, pending deposits, current
<RXUJHQHU OHQHUJ\XV JHG W IRUXSWRWZHQW\IRXUPRQWKV WQRJUH WHUOHYHORIGHW LOWK QPRQWKO\WRW OVZKLFKLVFXVWRPHUVSHFLÀF information that is collected from your  Electric
Electric  Natural Gas utility meter by your utility service provider.
Natural Gas utility meter by your utility service provider.
7KH ($3RIÀFHZLOOXVHWKLVLQIRUP WLRQWRKHOSGHWHUPLQH\RXUHOLJL LOLW\IRU QG VVLVW\RXLQ SSO\LQJWRS UWLFLS WHLQHQHUJ\ VVLVW QFH programs. If you authorize the disclosure, it will start on the date you sign this application and end when you terminate your participation in the relevant energy assistance program. You have a right to receive a copy of this form.
Please note that:
•You are not required to authorize your utility service provider to disclose your customer data.
•Your decision not to authorize the disclosure will not affect your utility services.
<RXUXWLOLW\VHUYLFHSURYLGHUP \QRWGLVFORVH\RXUFXVWRPHUG W H[FHSWLI\RX XWKRUL]HWKHGLVFORVXUHWRFRQWU FWHG JHQWVWK W perform services on behalf of the utility, or (3) as otherwise permitted or required by laws or regulations.
• Your utility service provider will have no control over the data disclosed pursuant to this consent, and will not be responsible for monitoring
RUW NLQJ Q\VWHSVWRHQVXUHWK WWKH ($3RIÀFHP LQW LQVWKHFRQÀGHQWL OLW\RIWKHG W RUXVHVWKHG W V XWKRUL]HG \\RX
3XUVX QWWRVHFWLRQ&56 ($3ZLOOQRWGLVFORVH Q\SULY WH SSOLF QWLQIRUP WLRQH[FHSWIRUWKHSXUSRVHRI GPLQLVWHULQJ SX OLF VVLVW QFH VGHÀQHG \6W WH QG)HGHU OO ZV QGUHJXO WLRQV
1 ($3LVWKH&RORU GR RZ,QFRPH(QHUJ\$VVLVW QFH3URJU P GPLQLVWHUHG \WKH&RORU GR'HS UWPHQWRI+XP Q6HUYLFHV QG ($3·V IÀOL WHV
O 11. SIGNATURE AND CONSENT
By signing below I understand, I acknowledge and agree that:
,I, PFRQW FWHG \ZH WKHUL] WLRQP\UHIXV OWRSHUPLWZH WKHUL] WLRQRIP\KRPHP \UHVXOWLQGHQL ORI ($3 HQHÀWV
0\6RFL O6HFXULW\1XP HUZLOO HXVHGWRUHTXHVW QGH[FK QJHLQIRUP WLRQZLWKRWKHU JHQFLHV VS UWRIWKHHOLJL LOLW\YHULÀF WLRQSURFHVV
3.The Colorado Department of Human Services (CDHS) may use my Social Security Number to get wage data, amount of unearned income, child
VXSSRUWF VH QGS \PHQWGLV XUVHPHQWUHFRUGVLQWHUHVWLQFRPH6RFL O6HFXULW\ HQHÀWVSHQVLRQVU LOUR GUHWLUHPHQWRUYHWHU Q·V HQHÀWV $VS UWRIWKHHOLJL LOLW\YHULÀF WLRQSURFHVVWKH&'+6K VP\SHUPLVVLRQWRFRQW FWRWKHU JHQFLHVRQP\ HK OIWRHVW OLVKHOLJL LOLW\
, PWKHFXVWRPHURIUHFRUGWKHFXVWRPHU·V XWKRUL]HG JHQWRU Q XWKRUL]HGWKLUGS UW\IRUWKHXWLOLW\VHUYLFH FFRXQWLGHQWLÀHGLQWKLV SSOLF WLRQ QG, XWKRUL]HP\XWLOLW\VHUYLFHSURYLGHUWRGLVFORVHP\FXVWRPHUG W VVSHFLÀHGLQVHFWLRQRIWKLV SSOLF WLRQ
<RXP \WHUPLQ WH\RXUFRQVHQWWRWKHGLVFORVXUHRI\RXUFXVWRPHUG W \\RXUXWLOLW\VHUYLFHSURYLGHUWRWKH ($3RIÀFH W Q\WLPH \ VHQGLQJ ZULWWHQUHTXHVWZLWK\RXUQ PH QGVHUYLFH GGUHVVWR\RXUXWLOLW\VHUYLFHSURYLGHULGHQWLÀHGLQVHFWLRQ
6.If LEAP repairs or replaces my heating system and I refuse to allow access to my dwelling for the purposes of completing the service
LQFOXGLQJ XWQRWOLPLWHGWRJRYHUQPHQWLQVSHFWLRQVUHTXLUHG \O ZWKLVUHIXV OP \UHVXOWLQGHQL ORI OO HQHÀWV
,WLV FULPHWROLHRQWKH SSOLF WLRQRUWRW NH HQHÀWVWK |
W,NQRZP\I PLO\ QG, UHQRWHOLJL OHWRUHFHLYH |
QG,P \ HVX MHFWWR |
FULPLQ OSURVHFXWLRQIRUNQRZLQJO\SURYLGLQJI OVHLQIRUP |
WLRQ*LYLQJI OVHLQIRUP WLRQP \ HSXQLVKHG \ |
ÀQHRIXSWR RU |
M LOWHUPRIXSWR\H UVRU RWK |
|
|
8.I declare that the information given by me in this application is true and correct. I understand the penalty for providing false information. $SHUVRQFRQYLFWHGRIIU XGXOHQW FWLYLW\F QQRWJHW ($3 VVLVW QFHIRUWKUHH\H UVIRUWKHÀUVWFRQYLFWLRQ QGSHUP QHQWO\IROORZLQJWKH second conviction.
W S I G N F U L L N A M E B E L O W W
|
Signature: __________________________________________________________ |
Date:________________ |
|
|
6LJQ WXUHRI$SSOLF |
QWPXVW HV PHSHUVRQOLVWHGLQ S JH |
0RQWK' \<H U |
|
|
|
If someone helped the applicant complete this application, such person must sign below. |
|
||
' WH |
||||
6LJQ WXUHRI+HOSHU |
$GGUHVV |
3KRQH |
||
If you would like to know the status of your application please call HEAT HELP at
Page 4 of 4 |
Completed |
| Fact Name | Description |
|---|---|
| Purpose of IML-4 Form | The IML-4 form is used for the Leap application, but specific details about its purpose cannot be determined as the form's contents were not provided. |
| Applicable Users | Without the form's contents, it's unclear who exactly should use the IML-4 form for the Leap application, whether businesses, individuals, or another group. |
| Governing Law(s) | The governing laws for the IML-4 form depend on its usage and jurisdiction, which cannot be identified without further context about the form's applications or the state(s) it pertains to. |
| Accessibility | Details on how users can access the IML-4 form for the Leap application cannot be confirmed without additional information about the distribution methods or platforms hosting the form. |
| Filing Procedure | Without the form's specifics, the exact procedure for filing the IML-4 form, including deadlines, submission methods, or required supporting documents, remains unclear. |
Once you've decided to submit the Leap application IML-4 form, understanding the next steps in the process is crucial. This guide will walk you through how to accurately complete the form, ensuring all your information is properly presented. After you submit the form, it will undergo a review process to ensure eligibility and completeness. It's essential to pay close attention to detail and provide all requested information to avoid delays in processing. Now, let's dive into the steps necessary to fill out your application.
After submitting the Leap application IML-4 form, the waiting period begins. The review committee will assess your application for completeness and eligibility. You might be contacted for further information or clarification. The decision process varies in time, so patience is essential. Stay proactive by checking your email and responding promptly to any inquiries from the review committee. Successfully navigating through these steps brings you closer to achieving your goals with the Leap program.
What is the Leap application IML-4 form?
The Leap application IML-4 form is a document used in the process of applying for a specific type of service or benefit through the Leap program. This form gathers essential information from applicants to ensure they meet the criteria for what they are applying for and to help the program make informed decisions on eligibility and the level of assistance to be provided.
Who needs to complete the IML-4 form?
Individuals seeking to avail themselves of the services or benefits offered by the Leap program must complete the IML-4 form. It's crucial for applicants to provide accurate and comprehensive information to facilitate a smooth application process and to enhance their chances of obtaining the needed assistance.
How can I obtain the IML-4 form?
The IML-4 form is generally available through the official Leap program website. Applicants can download the form directly from the site. Additionally, some local offices and agencies associated with the Leap program may have physical copies available for pick-up. It's advisable to contact these offices ahead of time to confirm availability.
What information do I need to provide on the IML-4 form?
The IML-4 form requires various pieces of information related to your personal identification, residence, financial situation, and the specific nature of the assistance you are seeking. This may include your full name, contact information, income details, and other relevant data that will help the program assess your application accurately.
Is assistance available for completing the IML-4 form?
Yes, assistance for completing the IML-4 form is often available. This support can come from various sources, including helpdesks or customer service teams associated with the Leap program. Sometimes, community organizations and legal aid services provide guidance and assistance to individuals filling out the form to ensure it is completed correctly.
What happens after I submit the IML-4 form?
After submission, your IML-4 form will be reviewed by the Leap program staff or the designated reviewing body. This process involves evaluating the information you've provided to determine your eligibility for the program. You may be contacted for additional information or to clarify the details you’ve submitted. Once the evaluation is complete, you will be informed of the decision regarding your application.
Can I appeal if my application is denied?
If your application is denied, you typically have the right to appeal the decision. The specific procedure for appeals will be outlined in the communication you receive about your application status. It's important to follow these instructions carefully and to submit your appeal within any specified deadlines to ensure your case is reconsidered.
Filling out the Leap application IML-4 form is a crucial step for individuals seeking assistance. However, several common mistakes can significantly hinder the process. One of the primary errors is not fully completing the form. Every question is designed to gather essential information. Incomplete answers can delay processing or lead to outright denial.
Another frequent mistake is providing incorrect information. This might seem obvious, but accuracy is paramount. Whether it's a simple typo in a name or date, or more significant errors like incorrect income figures, inaccuracies can complicate and extend the verification process.
Many applicants also overlook the necessity of attaching supporting documents. The IML-4 form requires specific documentation to verify the information provided. Failing to attach these documents, or submitting incomplete or unclear copies, can stall an application's progress.
Applicants often underestimate the importance of reading the instructions carefully. Every section of the IML-4 form comes with instructions aimed at clarifying what is needed. Ignoring these guidelines can lead to improperly filled sections, ultimately causing delays.
The use of ineligible handwriting is another oversight. While this might seem minor, illegible handwriting can lead to misinterpretation of critical details. It's always advisable to fill out the form using clear and legible handwriting, or better yet, type the information if the form format allows it.
A mistake that can easily be avoided is submitting the form without the necessary signatures. Signatures are a key component of the IML-4 form, serving as a personal attestation to the accuracy and truthfulness of the information provided. Missing signatures can invalidate the entire application.
Incorrectly calculating income and expenses is another common error. The IML-4 form often requires detailed financial information, and accuracy is crucial. Overestimating expenses or underestimating income can affect eligibility and the level of assistance provided.
Not updating personal information can also derail the application process. If contact information changes after submitting the IML-4 form, it's vital to inform the relevant authority immediately. Failure to do so can result in missed communications regarding the application status.
Submitting the form to the wrong office or agency is a mistake that can lead to significant delays. Each jurisdiction may have specific locations where the IML-4 form must be submitted. Misdirecting the form can mean it takes longer to reach the correct office, if it gets there at all.
Finally, waiting until the last minute to submit the form is a risky approach. Procrastination can lead to rushed applications, increasing the likelihood of errors. It's also important to consider the processing time required and to allow for any unforeseen delays.
In conclusion, careful attention to detail and thoroughness are crucial when filling out the Leap application IML-4 form. Avoiding these common mistakes can streamline the process, ensuring that the application is processed efficiently and accurately.
Filing a Leap application IML-4 form is a necessary step for certain legal procedures. However, to ensure a comprehensive approach, several other forms and documents often accompany the IML-4 form. Each of these supporting documents plays a vital role in the application process, serving to provide detailed information, confirm identity, or fulfill statutory requirements. Here are nine common forms and documents used alongside the IML-4 form.
Understanding and gathering these documents prior to filing can significantly streamline the application process. Each document serves a specific purpose, from establishing identity to providing evidence of financial stability. In the context of legal and administrative procedures, having a comprehensive collection of documents ready can expedite processes and enhance the likelihood of a favorable outcome.
The Leap application IML-4 form shares similarities with the Employment Eligibility Verification Form I-9. Both documents are designed to verify information crucial to determining eligibility - the IML-4 for program participants and the I-9 for employment purposes in the United States. Each form requires personal identification details and the submission of supporting documents to confirm the information provided is accurate and valid.
Another document akin to the IML-4 form is the Free Application for Federal Student Aid (FAFSA). Like the IML-4, the FAFSA gathers detailed personal and financial information from applicants to assess eligibility, in this case, for federal student financial aid. Both applications play pivotal roles in providing access to resources, demanding accuracy and completeness to ensure proper eligibility determination.
The Passport Application Form shares key characteristics with the IML-4 form, as both involve the collection of personal data to verify the applicant's identity and eligibility. While the IML-4 form may focus on program participation eligibility, the passport application is used to determine eligibility for a U.S. passport. Each requires the individual to provide personal history and identification documents to support their application.
The Medical History Form found in healthcare settings also mirrors the IML-4 form in certain respects. Both solicit detailed personal and history information - the IML-4 for program eligibility purposes and the Medical History Form for assessing patient health and creating treatment plans. Though the contexts differ, the emphasis on accurate, comprehensive information collection is common to both.
Similar to the IML-4 is the Tax Return Form, such as the IRS Form 1040, which collects detailed financial information from individuals to determine their tax liability or refund eligibility. Both forms require the individual to provide extensive details about their financial situation, although for different end purposes: the IML-4 for program eligibility and the 1040 for tax assessment.
The Voter Registration Form is another document sharing similarities with the IML-4. Both are gateways to civic engagement - the IML-4 by determining eligibility for a specific program and the Voter Registration Form by enabling participation in the electoral process. Each form collects personal identification information to verify the applicant's eligibility for the respective privileges.
Last, the Driver's License Application Form resembles the IML-4 in its purpose to gather personal information to verify eligibility, in this case, for a driver's license. Both applications entail the submission of personal and sometimes sensitive information to a governing body, requiring accuracy for proper assessment of eligibility and identification verification.
When filling out the Leap application IML-4 form, it's important to follow specific guidelines to ensure the process goes smoothly. Here are things you should and shouldn't do:
Do's:
Read the instructions carefully before you start filling out the form to make sure you understand all the requirements.
Gather all necessary documents and information before you begin, to ensure accuracy and completeness.
Use a blue or black pen if the form is being filled out by hand, to ensure the information is legible.
Answer all questions truthfully and to the best of your knowledge, as providing false information can result in penalties.
Double-check your answers for any mistakes or typos before submitting the form.
Keep a copy of the completed form for your records.
Contact the appropriate support service if you have any questions or need clarification on how to properly fill out the form.
Don'ts:
Don't leave any required fields blank. If a question doesn't apply, write "N/A" (not applicable) instead of leaving it empty.
Don't use corrections fluid or tape. If you need to make a correction, neatly cross out the mistake and write the correct information next to it or above it.
Don't submit the form without checking that all required signatures and dates are in place. Incomplete forms may be returned or rejected.
Don't provide false information or documents. This can lead to your application being rejected or legal action being taken against you.
Don't rush through the form. Taking your time can help prevent errors that could delay the processing of your application.
Don't forget to update your contact information if it changes after you've submitted the form, to ensure you can be reached if there are any questions or updates.
Don't hesitate to ask for help. If you're unsure about any part of the form, it's better to ask for clarification than to submit incorrect information.
There are several misconceptions about the Leap application IML-4 form that people often have. It's important to clear these up to ensure accurate completion and submission of the form. Here are ten common misconceptions:
When handling the Leap application IML-4 form, attention to detail and a clear understanding of the process are critical. To ensure accuracy and facilitate a smooth submission, consider the following key takeaways:
What Is I-20 - Students need to keep their I-20 form updated, especially if there are any changes in their program or personal information.
Notarized Letter of Consent - Informs about the consequences of providing false information or failing to adhere to the outlined commitments.