Fill a Valid Medication Administration Record Sheet Form
Fill a Valid Medication Administration Record Sheet Form
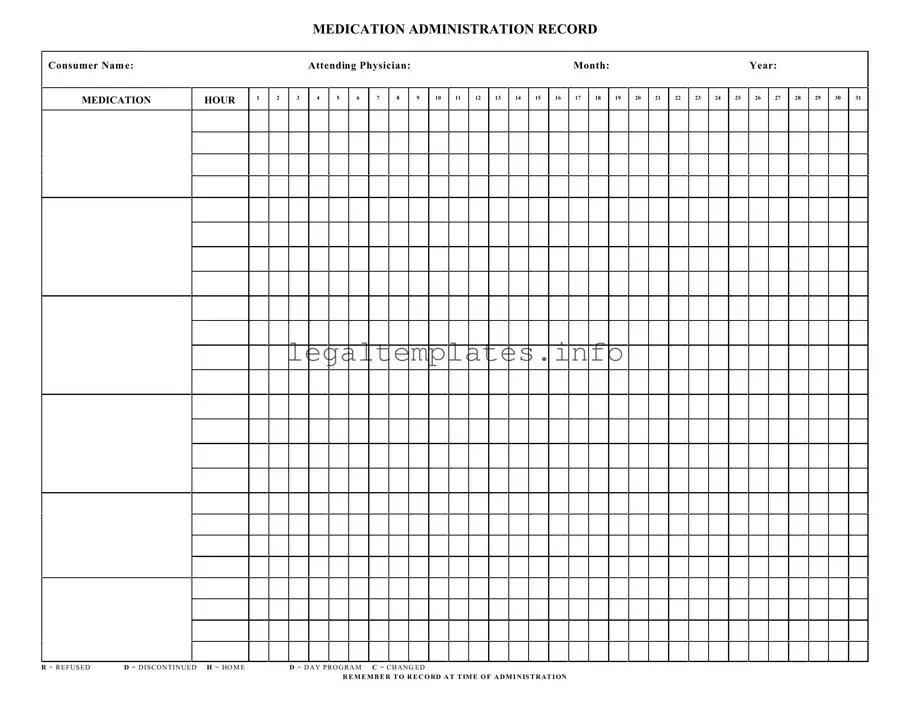
The Medication Administration Record Sheet serves as a critical document in managing and documenting the administration of medications to individuals in various healthcare settings. This detailed form includes essential information such as the consumer's name, the attending physician, and a comprehensive log that accounts for medication administration across the entire month, detailed down to each hour of the day. The sheet captures whether a medication was refused, discontinued, administered at home, during a day program, or if there were any changes in the medication regimen. Additionally represented by the notation 'R' for refused, 'D' for discontinued, 'H' for home, 'D' for day program, and 'C' for changes, this document plays a pivotal role in ensuring that healthcare providers and caretakers maintain accurate records of medication dispensation. Moreover, the directive to record at the time of administration underscores the form's importance in real-time medication management and adherence, thereby ensuring the well-being and safety of the consumer.
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
| Fact Name | Description |
|---|---|
| Purpose | The Medication Administration Record Sheet helps track the administration of medications to an individual over a specific period, ensuring accuracy and consistency in their care. |
| Key Components | It includes sections for the consumer's name, medication hour, attending physician, and a daily record for a month, with symbols for refused, discontinued, home, day program, and changes in medication. |
| Use of Symbols | Symbols like R (Refused), D (Discontinued), H (Home), and C (Changed) are utilized to quickly note the status of medication administration, making the sheet more efficient to use. |
| Importance of Accuracy | Accurate completion of the form is crucial for the health and safety of the consumer, affecting decisions made by healthcare providers and caregivers. |
| State-Specific Forms | While the basic structure is similar, some states may have specific requirements or additional fields in their Medication Administration Record Sheets, governed by state health laws. |
| Accessibility for Caregivers | The form is designed to be accessible and easy to use for caregivers and medical staff, ensuring all parties can accurately record and review medication administration. |
| Legal Relevance | Properly filled Medication Administration Record Sheets can serve as legal documents in case of disputes, demonstrating adherence to prescribed medications and protocols. |
Filling out a Medication Administration Record Sheet is an essential process in managing a patient's medication schedule to ensure accuracy and safety in drug administration. This document tracks the medication given to a consumer, capturing details such as the type of medication, dosage, and the times administered, along with any changes or refusal of medication. Precisely completing this form plays a critical role in maintaining an accurate record for healthcare providers to follow, ultimately contributing to the patient's well-being.
To properly fill out the Medication Administration Record Sheet, follow these steps:
Properly maintaining a Medication Administration Record Sheet is a systematic approach to pharmacological care, ensuring that patients receive their medications as prescribed. This diligence supports the integrity of their treatment plans and promotes positive health outcomes.
What is a Medication Administration Record Sheet (MAR)?
A Medication Administration Record Sheet, commonly referred to as an MAR, is a comprehensive report that tracks all the medication prescribed and administered to a patient over a period. It includes detailed information on the dosage, timing, and frequency of medication intake. This form is crucial in ensuring patients receive their medications correctly and safely, serving as a communication tool among healthcare providers.
Who needs to fill out the MAR?
Healthcare professionals such as nurses or caregivers who administer medications are primarily responsible for filling out the MAR. It's their duty to accurately record each instance of medication administration, including the time and any deviations from the prescribed regimen, like a missed dose or a patient refusal.
What do the abbreviations on the MAR mean (R, D, H, C)?
The abbreviations found on the MAR are critical for noting specific circumstances regarding medication administration. "R" stands for refused, indicating that a patient did not take a scheduled dose. "D" means discontinued, showing that the medication has been stopped. "H" signifies that the patient was at home, possibly explaining a missed dose in a care facility context. Lastly, "C" denotes a change in the medication, dosage, or timing.
Why is it important to record medication administration at the time of administration?
Recording medication administration at the time it occurs is vital for maintaining an accurate account of a patient's medication management. This real-time documentation helps prevent errors, such as double dosing or skipping a medication, ensuring the patient's safety. It also provides a clear record for any subsequent caregiver or healthcare provider that may be involved in the patient’s care.
Can modifications be made to the MAR?
Yes, modifications can be made to the MAR to reflect changes in a patient's medication regimen, such as dosage adjustments or new prescriptions. However, any changes should be made carefully and clearly, with the prior entry remaining legible. This ensures the continuity and accuracy of the medication record. Typically, any modifications should be verified and initialed by a healthcare professional.
What should be done if a medication error occurs?
In the event of a medication error, it's crucial to take immediate action to ensure the patient's safety. The error should be documented in the MAR, including what occurred and the steps taken afterward. Reporting the incident to the appropriate supervisor or healthcare provider for further assessment and response is also necessary. Learning from these incidents can help prevent future errors.
How long should MAR records be kept?
The retention period for MAR records varies depending on regulations and guidelines, which may differ by jurisdiction and type of healthcare facility. Generally, it's advised to keep these records for a significant period after the patient’s last entry to ensure that they can be referenced if there are questions about the patient’s medication history or any related legal matters. Consulting with facility policy or legal counsel can provide specific guidance.
What role does the MAR play in patient care?
The MAR plays a pivotal role in patient care by serving as a detailed ledger of a patient’s medication management. It aids in ensuring accuracy in medication administration, promoting patient safety, and facilitating clear communication among the healthcare team. The MAR also supports regulatory compliance and helps in the audit process by providing a clear history of medication administration practices.
When it comes to filling out the Medication Administration Record Sheet form, a common mistake is not correctly identifying the consumer. It's crucial that the consumer's name is accurately and legibly written to avoid any confusion, especially in settings where multiple records are managed.
Another area often overlooked is the section for the attending physician's name. This information is vital for ensuring that any medication administered is under the guidance of a responsible healthcare professional. Failure to provide or correctly spell the attending physician's name can lead to a lack of accountability and potential risks in care coordination.
The medication hour columns are marked from 1 to 31, intended for the days of the month. A frequent error is misinterpreting these columns to represent hours of the day, which can result in inaccurate medication schedules. Ensuring that each column is filled out according to the day of the month, not hour of the day, is key to maintaining the proper medication regimen.
Not recording the administration time of medications immediately is another mistake. The form has a clear reminder to "RECORD AT TIME OF ADMINISTRATION," yet this directive is often neglected. Timely documentation ensures an accurate medication timeline, which is crucial for monitoring effectiveness and preventing overdoses or missed doses.
Confusion also arises from the special codes (R = REFUSED, D = DISCONTINUED, H = HOME, D = DAY PROGRAM, C = CHANGED) used to note the status of the medication administration. Mistakes in understanding or using these codes can lead to incorrect interpretations of a patient's medication compliance and the current status of their prescriptions.
Ignoring to note changes in medication or administration details under the 'Change' column is another common oversight. Whenever there’s a change in the medication, dosage, or schedule, it must be documented to keep the record current. This documentation is vital for tracking the patient's response to certain medications and for future reference.
Omitting the month and year at the top of the form can lead to ambiguity, especially when records are being reviewed retrospectively. Accurate dating ensures that the medication administration is contextualized correctly over time.
Errors in medication names and dosages are all too common and perhaps among the most dangerous. Ensuring the correct medication name and dosage requires double-checking prescriptions and pharmacy instructions. An incorrect entry in these fields can have dire consequences for patient health.
Another frequent issue is the failure to mark medication refusal or discontinuation appropriately with the "R" or "D" codes. This neglection can lead to misunderstandings about a patient's medication compliance or the assumption that discontinued medications are still being taken.
Lastly, the form must be completed with attention to detail and clarity to avoid misinterpretation by other healthcare professionals. Illegible handwriting, incomplete information, and failure to update or maintain the record can significantly undermine patient care. Taking the time to fill out the form comprehensively and clearly is crucial for effective medication management.
When managing a patient's or individual's healthcare, especially in settings like nursing homes, hospitals, or assisted living facilities, the Medication Administration Record Sheet (MAR) is crucial. However, to ensure comprehensive care and appropriate medication management, several other forms and documents are frequently used in tandem with the MAR. These documents help in monitoring the patient's overall health condition, recording specific medical information, and ensuring that the administration of medication and healthcare services are accurately tracked and optimized for the patient's well-being.
Together with the Medication Administration Record Sheet, these documents form a comprehensive system for managing a patient's or individual's medication and overall health care. This system not only supports healthcare providers in delivering high-quality care but also ensures the safety and well-being of patients by meticulously tracking their treatment and responses to medication. By maintaining and regularly reviewing these documents, healthcare providers can make informed decisions, prevent possible medication errors, and provide personalized and effective care.
The Medication Administration Record Sheet form shares notable similarities with a Pain Management Journal. Both documents are invaluable in tracking and documenting a specific aspect of a patient's care over a designated period. A Pain Management Journal typically involves chronological entries outlining the efficacy of pain control measures, similar to how the Medication Administration Record tracks the administration, effects, and any refusal or changes in medication dosages for individuals. Each entry helps healthcare providers make informed decisions regarding the continuation, discontinuation, or adjustment of treatment plans.
Another document akin to the Medication Administration Record is the Blood Glucose Monitoring Chart. This chart is used by individuals with diabetes to record their blood sugar levels at various times of the day, creating a comprehensive overview of how well their diabetes is being managed. The parallel with the Medication Administration Record lies in the systematic recording of crucial health metrics intended to guide therapeutic decisions. Both documents serve as a communication tool among healthcare providers, offering a snapshot of the patient's current state and signaling when adjustments are necessary.
The Patient Progress Notes is similarly structured to the Medication Administration Record, providing sequential documentation but with a broader focus. It encompasses all aspects of patient care, including but not limited to, responses to medication. The Progress Notes serve as a storyline of the patient's journey through treatment, including observations made by healthcare providers, the effectiveness of interventions, and any side effects or complications that arise. This document, like the Medication Administration Record, is essential for ensuring continuity of care and facilitating the evaluation of treatment efficacy.
The Vaccine Administration Record (VAR) also mirrors the structure of the Medication Administration Record, even though it is specifically tailored towards tracking vaccinations. It details the administration of each vaccine, including the date, type, and any adverse reactions, which is crucial for managing public health and ensuring individual patient care. Like the Medication Administration Record, the VAR is fundamental in preventing medication errors, tracking patient compliance, and facilitating communication among healthcare professionals to ensure that an individual's vaccination schedule is up-to-date and effective.
When managing medications for individuals, especially in settings requiring meticulous documentation like healthcare facilities or for individuals with complex care needs, the Medication Administration Record (MAR) Sheet is a crucial tool. Understanding the dos and don'ts of filling out this form can prevent medication errors, ensure compliance with regulations, and foster safe, effective care. Here are essential tips for correctly completing the MAR Sheet.
By adhering to these guidelines, those responsible for medication administration can foster a safer environment for consumers, reducing the risk of medication errors while enhancing the quality of care provided.
When it comes to Medication Administration Record (MAR) Sheets, there are several misconceptions that can potentially impact the quality of care and safety of consumers. Clarifying these misconceptions is vital for healthcare professionals and caretakers who handle medication administration. Below are some common misunderstandings about the MAR Sheet:
This is inaccurate as the MAR Sheet is a critical tool for all healthcare professionals involved in administering medication, including but not limited to nurses. It can also be used by pharmacists, certified nursing assistants, and other caretakers who are authorized to administer medications.
While eMARs are increasingly common and offer advantages like decreased errors and easier tracking, paper-based MAR Sheets are still in use, especially in settings with limited access to digital resources.
For accurate medication history and accountability, discontinued medications should remain on the MAR Sheet with a clear notation (e.g., "D" for discontinued), rather than being removed or obliterated.
Pharmacists play a crucial role in the medication administration process, including reviewing MAR Sheets for potential drug interactions, allergies, or dosing errors. Their review is an essential check in the medication administration process.
It is essential to document when a consumer refuses a medication ("R" for refused) on the MAR Sheet. This information is critical for health care providers to understand medication compliance and to assess the need for alternative treatments or interventions.
While the attending physician prescribes medication, pharmacists and nurses also have the authority to make certain annotations for clarity, corrections, or to note discontinuations after consultation with the physician, ensuring the MAR Sheet is accurate and up-to-date.
It is critical to record all medications administered, including those given at home ("H" for home), on the MAR Sheet. This ensures continuity of care and accurate medication tracking regardless of the administration setting.
For consistency and to avoid misunderstandings, only standard notations and symbols specified on the MAR Sheet should be used. Using unauthorized shorthand or symbols can lead to errors in medication administration.
Correcting these misconceptions is crucial for the safety and well-being of consumers under care. Understanding the proper use and importance of the Medication Administration Record Sheet is fundamental for all individuals involved in the medication administration process.
The Medication Administration Record Sheet is an essential tool in ensuring the safe and proper administration of medications to an individual, particularly in a healthcare setting or for individuals under care management. Understanding the correct way to fill out and use this form is paramount for the health and safety of the consumer. Here are nine key takeaways regarding the proper utilization of this form:
Proper use of the Medication Administration Record Sheet facilitates effective communication among caregivers and healthcare providers, ensuring that individuals receive the correct medications at the right times, ultimately promoting better health outcomes.
Cg 2010 - It offers a mechanism for ensuring that additional insureds have the necessary liability protection without the need for separate policies.
P-45 - The tax code at the leaving date is noted to determine how future income should be taxed.
Texas Odometer Disclosure Statement - Affords protection against fraud by requiring detailed vehicle identification and mileage disclosure.