Fill a Valid Medication Count Sheet Form
Fill a Valid Medication Count Sheet Form
In the meticulous and often fast-paced environment of healthcare facilities, keeping accurate records of medication administration is paramount. The Medication Count Sheet form plays a crucial role in this process, ensuring that patients receive their medications correctly and safely. This form, utilized by healthcare providers, tracks multiple critical details: the resident or patient for whom the medication is prescribed; the quantity of the medication at the start; the specific dates and times the medication is administered; the drug’s strength; and the staff member’s signature who administered the drug. Additionally, it helps in maintaining an ongoing record of the quantity of medication remaining, which is essential for inventory control and preventing medication errors. By providing a structured and clear format for recording these details, the Medication Count Sheet form acts as a vital tool in the management of medication within healthcare settings, contributing to patient safety and effective healthcare delivery.
|
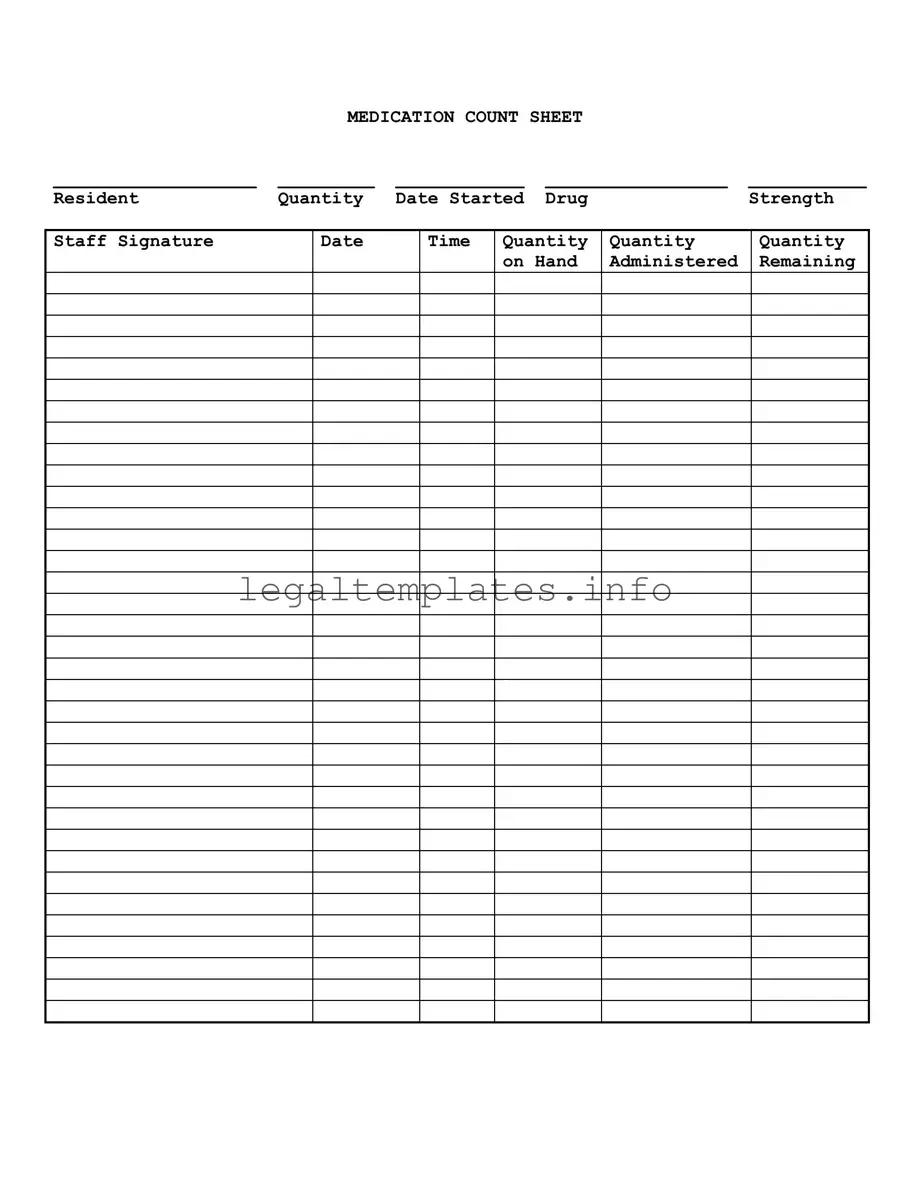
MEDICATION COUNT SHEET |
|
||
___________________ |
_________ |
____________ |
_________________ |
___________ |
Resident |
Quantity |
Date Started |
Drug |
Strength |
Staff Signature
Date
Time
Quantity |
Quantity |
Quantity |
on Hand |
Administered |
Remaining |
|
|
|
| Fact Name | Description |
|---|---|
| Purpose of Form | The Medication Count Sheet is used to track the medication administered to a resident, ensuring accurate dosage and accountability. |
| Key Components | Important fields include Resident, Quantity, Date Started, Drug Strength, Staff Signature, Date, Time, Quantity Administered, and Quantity Remaining. |
| Record Keeping | This form plays a critical role in maintaining detailed records for each resident’s medication management, aiding in consistency and safety. |
| Staff Accountability | By signing the form, staff members acknowledge their responsibility in administering the medication accurately and verifying the count. |
| Regulatory Compliance | Using a Medication Count Sheet helps healthcare facilities comply with state and federal regulations concerning drug administration. |
| Error Prevention | The form is a critical tool in reducing medication errors, ensuring patients receive the correct dosage at the correct time. |
| Auditing Tool | These records can be audited by healthcare supervisors or inspectors to ensure proper medication management practices are followed. |
| Legal Protection | Maintaining accurate medication records can serve as evidence of proper care in legal disputes or investigations. |
| Governing Laws | While specifics can vary, most US states have health and public safety laws that govern the administration of medication within care facilities. |
Filling out a Medication Count Sheet is a critical task for managing and documenting the medication supply for a resident. This straightforward process involves entering information about the resident's medication, including the quantity on hand, dates, times, and amounts administered, ensuring accurate tracking and accountability. Follow these steps to complete the form correctly.
Following these steps will help maintain a precise and up-to-date medication log, critical for the well-being of the resident and compliance with health management protocols.
What is a Medication Count Sheet?
A Medication Count Sheet is a document used in healthcare settings, particularly in residential care facilities, to track and record the dispensation of medication to individuals. It serves as a detailed log, noting the resident's name, the quantity of medication on hand, the start date, the drug name, its strength, and the signature of the staff administering the medicine. Additionally, it records the date, time, quantity administered, and the remaining quantity of medication to ensure accuracy in dosage and to prevent errors.
How do you fill out the Medication Count Sheet?
To fill out the Medication Count Sheet correctly, one must start by entering the resident's name at the top of the form. Following this, the quantity of the medication currently on hand is noted. Then, information about the medication, including the start date, drug name, and its strength, is filled in. Each time the medication is administered, the staff member responsible must record the date and time of administration, the quantity of the medication given to the resident, and the new quantity remaining. Staff members must also sign their names to verify that the information is accurate and the medication has been given as detailed.
Why is it important to use a Medication Count Sheet?
Using a Medication Count Sheet is fundamental in ensuring the health and safety of residents in care facilities. It helps prevent medication errors, which can lead to adverse drug reactions or failures in treatment. By keeping a meticulous record of medication dispensation, care providers can monitor and verify that residents are receiving the correct dosages at the proper times. It also provides a clear audit trail for healthcare providers, regulatory bodies, and families, offering transparency and accountability in the administration of medication.
What should you do if you notice discrepancies in the Medication Count Sheet?
If discrepancies are noticed in the Medication Count Sheet, it is crucial to act immediately. First, verify the records to determine the nature of the discrepancy, whether it is a recording error or a medication mishandling situation. Notify the supervisor or the healthcare provider in charge to investigate the issue further. It may be necessary to review the medication administration protocols, check against other documentation, and possibly speak with the staff involved. Taking prompt and appropriate action can help prevent medication errors and ensure resident safety.
When it comes to managing medication for residents in various settings, the Medication Count Sheet plays a crucial role in ensuring accuracy and accountability. However, there are common pitfalls that can lead to errors in medication management. Understanding these mistakes can greatly improve the effectiveness of medication tracking and administration.
One common mistake is not double-checking the resident's name when filling out the form. This may seem like a basic step, but in busy settings, it's easy to mix up sheets or overlook discrepancies. This can lead to administering medication to the wrong resident, which is both dangerous and a violation of trust.
Another error is incorrectly recording the quantity of medication on hand at the start. This initial count is the foundation for all future entries on the sheet, and inaccuracies can cascade, leading to confusion about whether medications have been administered properly or even prompting concerns about medication security.
Often, staff may rush and forget to record the date and time when medication is administered. This oversight can complicate efforts to track when the last dose was given, which is especially critical for medications that must be spaced out precisely to maintain their effectiveness.
A lack of consistency in how the staff signature is recorded is yet another mistake. Inconsistent or missing signatures make it difficult to verify who administered medication, complicating accountability and potentially hindering follow-up in case of an adverse reaction or other issues.
Failing to accurately note the quantity of medication administered is a significant error. Whether it's giving too much, too little, or failing to record the dose accurately, such mistakes can have serious health implications for residents and legal ramifications for the facility.
Not updating the quantity remaining after each administration is a critical oversight. This information is essential for knowing when to reorder medication and for preventing either stock-outs or overstocking, which can lead to medication wastage or misuse.
Omitting or incorrectly filling out the drug strength field can lead to errors in medication administration, especially in settings where a medication comes in multiple strengths. Administering the wrong strength of a medication can have substantial consequences for patient health.
Ignoring or inaccurately tracking the date the medication was started is yet another common error. This information is pivotal for determining the course of treatment and ensuring that medication is administered within its effective date range and discontinued appropriately.
Last but not least, a simple yet impactful mistake is the failure to regularly review and reconcile the Medication Count Sheet with the actual medication stock. Regular checks can prevent many of the aforementioned errors from becoming problematic, ensuring both the health and safety of the resident and regulatory compliance for the facility.
By being mindful of these common mistakes and taking steps to avoid them, staff can greatly improve the accuracy and reliability of medication administration, ultimately ensuring better care for their residents.
In the meticulous realm of healthcare and medication administration, especially in settings like nursing homes, rehabilitation centers, and home care, the Medication Count Sheet form plays a pivotal role in ensuring the accurate tracking of medication dosages given to residents. However, to paint a full picture of a patient's medication management and adherence, several other essential documents typically accompany this form. These complementary forms are crucial for providing a comprehensive overview, ensuring both the safety and well-being of the patient and compliance with regulatory standards.
Together, these documents form the backbone of an efficient and safe medication management system. By integrating the Medication Count Sheet with the Medication Administration Record, Treatment Administration Record, Controlled Substance Log, and Patient-Specific Orders, healthcare providers can ensure a holistic approach to patient care. This not just mitigates risks associated with medication errors but also enhances the overall effectiveness of the treatment plans, paving the way for optimal health outcomes.
The Medication Count Sheet shares similarities with the Controlled Substance Log. Both documents involve meticulous record-keeping related to the administration and inventory of medications. Just as a Medication Count Sheet tracks the quantity of medication on hand, doses administered, and remaining quantities, the Controlled Substance Log specifically focuses on controlled substances, monitoring their usage, inventory levels, and any discrepancies to ensure compliance with regulations. These logs are critical in healthcare settings for managing medication safely and preventing misuse.
Another document akin to the Medication Count Sheet is the Patient Medication Profile. This document outlines all medications prescribed to a specific patient, including drug name, strength, and dosing instructions. While the Medication Count Sheet focuses on the inventory and administration records of medications, the Patient Medication Profile provides a comprehensive view of a patient's prescribed medications. This ensures healthcare providers have a full understanding of a patient's medication regimen, facilitating better care coordination and drug therapy management.
The Drug Dispensing Log also shares similarities with the Medication Count Sheet. This log records every instance of medication dispensed to patients, often found in pharmacies or hospitals. It includes details such as the patient’s name, the dispensed drug's name, quantity, date, and the dispensing pharmacist’s signature. Like the Medication Count Sheet, it serves to document the usage and movement of medications comprehensively but from the dispensing perspective, ensuring accountability and accuracy in the dispensing process.
A Vaccine Administration Record (VAR) is similar to the Medication Count Sheet in its function of documenting the administration of vaccines to patients. The VAR records essential details such as patient identification, vaccine name, dose, lot number, and date and time of administration, much like the Medication Count Sheet notes the detailed tracking of medication usage. Both documents are integral in upholding patient safety, ensuring proper vaccine and medication management, and adherence to treatment and immunization schedules.
Finally, the Inventory Control Sheet for Pharmacy parallels the Medication Count Sheet, but with a broader focus on managing all pharmacy inventory, not just medications given to specific individuals. This sheet helps in tracking medication stock levels, reordering needs, and expiration dates, similar to how the Medication Count Sheet tracks the quantities of specific medications in relation to patient administration. Both forms are essential in maintaining the accuracy of pharmacy inventory and ensuring medications are available and safe for patient use.
Filling out a Medication Count Sheet is a crucial process in ensuring the proper management of medication for residents in a care setting. Attention to detail and accuracy are paramount. Here are some guidelines to help ensure the form is completed correctly and effectively.
By following these guidelines, staff can help maintain a high standard of care, reduce the risk of medication errors, and enhance the overall safety and well-being of residents. Accurate completion of the Medication Count Sheet is a critical component of effective medication management in care settings.
A Medication Count Sheet is an essential tool in managing and tracking the administration of drugs for residents in healthcare facilities. However, there are several misconceptions about its use and importance. Let's clarify some of these misunderstandings.
It is solely for hospital use: Many believe that Medication Count Sheets are only for hospitals. However, they are vital in various settings, including nursing homes, assisted living facilities, and even for personal use at home for those managing complex medication regimens.
It's too complicated for non-medical staff: While it involves medical information, the form is designed to be straightforward. With proper training, non-medical staff, caregivers, and family members can accurately maintain this sheet, ensuring the safety and well-being of the individual under care.
Only prescription medications need to be counted: This is a common misconception. Over-the-counter medications, vitamins, and supplements should also be included if they are part of the individual's care plan, as interactions with prescription medications can impact a resident's health.
Digital records have made it obsolete: Although digital solutions are increasingly used for medication management, the Medication Count Sheet remains a crucial, fail-safe document. It serves as an immediate, accessible record, especially important in emergency situations or when digital systems fail.
Any staff member can manage it: While it's true that various staff members can be trained to update the sheet, the responsibility of managing and reviewing it should fall on qualified healthcare professionals. They can accurately interpret and act on the information to ensure optimal care.
It's mainly for legal protection: While it does provide a legal record of medication administration, its primary purpose is to ensure the safety and health of the resident. It fosters communication among caregivers about the ongoing care and treatment of an individual.
Errors are difficult to correct: Mistakes can and do happen. However, there are protocols for correcting errors on a Medication Count Sheet. The key is to document any corrections clearly and have them verified by a supervising healthcare professional to maintain the integrity of the record.
When managing medications within a healthcare setting, the utilization of a Medication Count Sheet is pivotal for ensuring accuracy, safety, and compliance with regulatory standards. The following key takeaways have been designed to equip professionals with a foundational understanding of how to effectively fill out and use this form:
Effective management of the Medication Count Sheet not only supports the health and safety of residents but also reinforces best practices within medicinal administration. It acts as a critical tool in the careful monitoring and control of medication usage, serving as a safeguard against errors and a source of essential data for healthcare providers. Emphasis on meticulous documentation and adherence to the protocols outlined above ensures operational integrity and contributes significantly to the overall quality of care.
Generic Bill of Lading - A form that specifies the terms and conditions under which goods are moved from one location to another.
Prescription Bottle Label Requirements - Includes the pharmacy's contact information for patient queries or concerns regarding the medication.